As the world struggles to control Coronavirus (COVID-19,) U.S. health officials are refighting battles they thought they had won, such as halting measles outbreaks, reducing deaths from heart disease and protecting young people from tobacco.
For much of the 20th century, medical progress seemed limitless.
Antibiotics revolutionized the care of infections. Vaccines turned deadly childhood diseases into distant memories. Americans lived longer, healthier lives than their parents.
Even as the world struggles to control a mysterious new viral illness known as COVID-19, U.S. health officials are refighting battles they thought they had won, such as halting measles outbreaks, reducing deaths from heart disease and protecting young people from tobacco. These hard-fought victories are at risk as parents avoid vaccinating children, obesity rates climb, and vaping spreads like wildfire among teens.
Things looked promising for American health in 2014, when life expectancy hit 78.9 years. Then, life expectancy declined for three straight years — the longest sustained drop since the Spanish flu of 1918, which killed about 675,000 Americans and 50 million people worldwide, said Dr. Steven Woolf, a professor of family medicine and population health at Virginia Commonwealth University.
Although life expectancy inched up slightly in 2018, it hasn’t yet regained the lost ground, according to the Centers for Disease Control and Prevention.
“These trends show we’re going backwards,” said Dr. Sadiya Khan, an assistant professor of cardiology and epidemiology at Northwestern University Feinberg School of Medicine.
While the reasons for the backsliding are complex, many public health problems could have been avoided, experts say, through stronger action by federal regulators and more attention to prevention.
“We’ve had an overwhelming investment in doctors and medicine,” said Dr. Sandro Galea, dean of the Boston University School of Public Health. “We need to invest in prevention — safe housing,good schools, living wages, clean air and water.”
Superbugs — resistant to even the strongest antibiotics — threaten to turn back the clock on the treatment of infectious diseases. Resistance occurs when bacteria and fungi evolve in ways that let them survive and flourish, in spite of treatment with the best available drugs. Each year, resistant organisms cause more than 2.8 million infections and kill more than 35,000 people in the U.S.
With deadly new types of bacteria and fungi ever emerging, Dr. Robert Redfield, the CDC director, said the world has entered a “post-antibiotic era.” Half of all new gonorrhea infections, for example, are resistant to at least one type of antibiotic, and the CDC warns that “little now stands between us and untreatable gonorrhea.”
That news comes as the CDC also reports a record number of combined cases of gonorrhea, syphilis and chlamydia, which were once so easily treated that they seemed like minor threats compared with HIV.
The United States has seen a resurgence of congenital syphilis, a scourge of the 19th century, which increases the risk of miscarriage, permanent disabilities and infant death. Although women and babies can be protected with early prenatal care, 1,306 newborns were born with congenital syphilis in 2018 and 94 of them died, according to the CDC.
Those numbers illustrate the “failure of American public health,” said Dr. Cornelius “Neil” Clancy, a spokesperson for the Infectious Diseases Society of America. “It should be a global embarrassment.”
The proliferation of resistant microbes has been fueled by overuse, by doctors who write unnecessary prescriptions as well as farmers who give the drugs to livestock, said Dr. William Schaffner, a professor of preventive medicine at Vanderbilt University Medical Center in Nashville, Tennessee.
Although new medications are urgently needed, drug companies are reluctant to develop antibiotics because of the financial risk, said Clancy, noting that two developers of antibiotics recently went out of business. The federal government needs to do more to make sure patients have access to effective treatments, he said. “The antibiotic market is on life support,” Clancy said. “That shows the real perversion in how the health care system is set up.”
A Slow Decline
A closer look at the data shows that American health was beginning to suffer 30 years ago. Increases in life expectancy slowed as manufacturing jobs moved overseas and factory towns deteriorated, Woolf said.
By the 1990s, life expectancy in the United States was falling behind that of other developed countries.
The obesity epidemic, which began in the 1980s, is taking a toll on Americans in midlife, leading to diabetes and other chronic illnesses that deprive them of decades of life. Although novel drugs for cancer and other serious diseases give some patients additional months or even years, Khan said, “the gains we’re making at the tail end of life cannot make up for what’s happening in midlife.”
Progress against overall heart disease has stalled since 2010. Deaths from heart failure — which can be caused by high blood pressure and blocked arteries around the heart — are rising among middle-aged people. Deaths from high blood pressure, which can lead to kidney failure, also have increased since 1999.
“It’s not that we don’t have good blood pressure drugs,” Khan said. “But those drugs don’t do any good if people don’t have access to them.”
Addicting A New Generation
While the United States never declared victory over alcohol or drug addiction, the country has made enormous progress against tobacco. Just a few years ago, anti-smoking activists were optimistic enough to talk about the “tobacco endgame.”
Today, vaping has largely replaced smoking among teens, said Matthew Myers, president of the Campaign for Tobacco-Free Kids. Although cigarette use among high school students fell from 36% in 1997 to 5.8% today, studies show 31% of seniors used electronic cigarettes in the previous month.
FDA officials say they’ve taken “vigorous enforcement actions aimed at ensuring e-cigarettes and other tobacco products aren’t being marketed or sold to kids.” But Myers said FDA officials were slow to recognize the threat to children.
With more than 5 million teens using e-cigarettes, Myers said, “more kids are addicted to nicotine today than at any time in the past 20 years. If that trend isn’t reversed rapidly and dynamically, it threatens to undermine 40 years of progress.”
Ignoring Science
Where children live has long determined their risk of infectious disease. Around the world, children in the poorest countries often lack access to lifesaving vaccines.
Yet in the United States — where a federal program provides free vaccines — some of the lowest vaccination rates are in affluent communities, where some parents disregard the medical evidence that vaccinating kids is safe.
Studies show that vaccination rates are drastically lower in some private schools and “holistic kindergartens” than in public schools.
It could be argued that vaccines have been a victim of their own success.
Before the development of a vaccine in the 1960s, measles infected an estimated 4 million Americans a year, hospitalizing 48,000, causing brain inflammation in about 1,000 and killing 500, according to the CDC.
“Now, mothers say, ‘I don’t see any measles. Why do we have to keep vaccinating?’” Schaffner said. “When you don’t fear the disease, it becomes very hard to value the vaccine.”
Last year, a measles outbreak in New York communities with low vaccination rates spread to almost 1,300 people — the most in 25 years — and nearly cost the country its measles elimination status. “Measles is still out there,” Schaffner said. “It is our obligation to understand how fragile our victory is.”
Health-Wealth Disparities
To be sure, some aspects of American health are getting better.
Cancer death rates have fallen 27% in the past 25 years, according to the American Cancer Society. The teen birth rate is at an all-time low; teen pregnancy rates have dropped by half since 1991, according to the Department of Health and Human Services. And HIV, which was once a death sentence, can now be controlled with a single daily pill. With treatment, people with HIV can live into old age.
Yet the health gap has grown wider in recent years. Life expectancy in some regions of the country grew by four years from 2001 to 2014, while it shrank by two years in others, according to a 2016 study in JAMA.
The gap in life expectancy is strongly linked to income: The richest 1% of American men live 15 years longer than the poorest 1%; the richest women live 10 years longer than the poorest, according to the JAMA study.
“We’re not going to erase that difference by telling people to eat right and exercise,” said Dr. Richard Besser, CEO of the Robert Wood Johnson Foundation and former acting director of the CDC. “Personal choices are part of it. But the choices people make depend on the choices they’re given. For far too many people, their choices are extremely limited.”
The infant mortality rate of black babies is twice as high as that of white newborns, according to the Department of Health and Human Services. Babies born to well-educated, middle-class black mothers are more likely to die before their 1st birthday than babies born to poor white mothers with less than a high school education, according to a report from the Brookings Institution.
In trying to improve American health, policymakers in recent years have focused largely on expanding access to medical care and encouraging healthy lifestyles. Today, many advocate taking a broader approach, calling for systemic change to lift families out of the poverty that erodes mental and physical health.
Several policies have been shown to improve health.
Children who receive early childhood education, for example, have lower rates of obesity, child abuse and neglect, youth violence and emergency department visits, according to the CDC.
And earned income tax credits — which provide refunds to lower-income people — have been credited with keeping more families and children above the poverty line than any other federal, state or local program, according to the CDC. Among families who receive these tax credits, mothers have better mental health and babies have lower rates of infant mortality and weigh more at birth, a sign of health.
Improving a person’s environment has the potential to help them far more than writing a prescription, said John Auerbach, president and CEO of the nonprofit Trust for America’s Health.
“If we think we can treat our way out of this, we will never solve the problem,” Auerbach said. “We need to look upstream at the underlying causes of poor health.”
Beeler worried that a failed drug test — even if it was for a medication to treat his addiction (like buprenorphine) — would land him in prison.
She was in medical school. He was just out of prison.
Sarah Ziegenhorn and Andy Beeler’s romance grew out of a shared passion to do more about the country’s drug overdose crisis.
Ziegenhorn moved back to her home state of Iowa when she was 26. She had been working in Washington, D.C., where she also volunteered at a needle exchange — where drug users can get clean needles. She was ambitious and driven to help those in her community who were overdosing and dying, including people she had grown up with.
“Many people were just missing because they were dead,” said Ziegenhorn, now 31. “I couldn’t believe more wasn’t being done.”
She started doing addiction advocacy in Iowa City while in medical school — lobbying local officials and others to support drug users with social services.
Beeler had the same conviction, born from his personal experience.
“He had been a drug user for about half of his life — primarily a longtime opiate user,” Ziegenhorn said.
Beeler spent years in and out of the criminal justice system for a variety of drug-related crimes, such as burglary and possession. In early 2018, he was released from prison. He was on parole and looking for ways to help drug users in his hometown.
He found his way to advocacy work and, through that work, found Ziegenhorn. Soon they were dating.
“He was just this really sweet, no-nonsense person who was committed to justice and equity,” she said. “Even though he was suffering in many ways, he had a very calming presence.”
People close to Beeler describe him as a “blue-collar guy” who liked motorcycles and home carpentry, someone who was gentle and endlessly curious. Those qualities could sometimes hide his struggle with anxiety and depression. Over the next year, Beeler’s other struggle, with opioid addiction, would flicker around the edges of their life together.
Eventually, it killed him.
People on parole and under supervision of the corrections system can face barriers to receiving appropriate treatment for opioid addiction. Ziegenhorn said she believes Beeler’s death is linked to the many obstacles to medical care he experienced while on parole.
About 4.5 million people are on parole or probation in the U.S., and research shows that those under community supervision are much more likely to have a history of substance use disorder than the general population. Yet rules and practices guiding these agencies can preclude parolees and people on probation from getting evidence-based treatment for their addiction.
A Shared Passion For Reducing Harm
From their first meeting, Ziegenhorn said, she and Beeler were in sync, partners and passionate about their work in harm reduction — public health strategies designed to reduce risky behaviors that can hurt health.
After she moved to Iowa, Ziegenhorn founded a small nonprofit called the Iowa Harm Reduction Coalition. The group distributes the opioid-overdose reversal drug naloxone and other free supplies to drug users, with the goal of keeping them safe from illness and overdose. The group also works to reduce the stigma that can dehumanize and isolate drug users. Beeler served as the group’s coordinator of harm reduction services.
“In Iowa, there was a feeling that this kind of work was really radical,” Ziegenhorn said. “Andy was just so excited to find out someone was doing it.”
Meanwhile, Ziegenhorn was busy with medical school. Beeler helped her study. She recalled how they used to take her practice tests together.
“Andy had a really sophisticated knowledge of science and medicine,” she said. “Most of the time he’d been in prison and jails, he’d spent his time reading and learning.”
Beeler was trying to stay away from opioids, but Ziegenhorn said he still used heroin sometimes. Twice she was there to save his life when he overdosed. During one episode, a bystander called the police, which led to his parole officer finding out.
“That was really a period of a lot of terror for him,” Ziegenhorn said.
Beeler was constantly afraid the next slip — another overdose or a failed drug test — would send him back to prison.
An Injury, A Search For Relief
A year into their relationship, a series of events suddenly brought Beeler’s history of opioid use into painful focus.
It began with a fall on the winter ice. Beeler dislocated his shoulder — the same one he’d had surgery on as a teenager.
“At the emergency room, they put his shoulder back into place for him,” Ziegenhorn said. “The next day it came out again.”
She said doctors wouldn’t prescribe him prescription opioids for the pain because Beeler had a history of illegal drug use. His shoulder would dislocate often, sometimes more than once a day.
“He was living with this daily, really severe constant pain — he started using heroin very regularly,” Ziegenhorn said.
Beeler knew what precautions to take when using opioids: Keep naloxone on hand, test the drugs first and never use alone. Still, his use was escalating quickly.
A Painful Dilemma
The couple discussed the future and their hope of having a baby together, and eventually Ziegenhorn and Beeler agreed: He had to stop using heroin.
They thought his best chance was to start on a Food and Drug Administration-approved medication for opioid addiction, such as methadone or buprenorphine. Methadone is an opioid, and buprenorphine engages many of the same opioid receptors in the brain; both drugs can curb opioid cravings and stabilize patients. Studies show daily maintenance therapy with such treatment reduces the risks of overdose and improves health outcomes.
But Beeler was on parole, and his parole officer drug-tested him for opioids and buprenorphine specifically. Beeler worried that if a test came back positive, the officer might see that as a signal that Beeler had been using drugs illegally.
Ziegenhorn said Beeler felt trapped: “He could go back to prison or continue trying to obtain opioids off the street and slowly detox himself.”
He worried that a failed drug test — even if it was for a medication to treat his addiction — would land him in prison. Beeler decided against the medication.
A few days later, Ziegenhorn woke up early for school. Beeler had worked late and fallen asleep in the living room. Ziegenhorn gave him a kiss and headed out the door. Later that day, she texted him. No reply.
She started to worry and asked a friend to check on him. Not long afterward, Beeler was found dead, slumped in his chair at his desk. He’d overdosed.
“He was my partner in thought, and in life and in love,” Ziegenhorn said.
It’s hard for her not to rewind what happened that day and wonder how it could have been different. But mostly she’s angry that he didn’t have better choices.
“Andy died because he was too afraid to get treatment,” she said.
Beeler was services coordinator for the Iowa Harm Reduction Coalition, a group that works to help keep drug users safe. A tribute in Iowa City after his death began, “He died of an overdose, but he’ll be remembered for helping others avoid a similar fate.” (COURTESY OF SARAH ZIEGENHORN)
How Does Parole Handle Relapse? It Depends
It’s not clear that Beeler would have gone back to prison for admitting he’d relapsed and was taking treatment. His parole officer did not agree to an interview.
But Ken Kolthoff, who oversees the parole program that supervised Beeler in Iowa’s First Judicial District Department of Correctional Services, said generally he and his colleagues would not punish someone who sought out treatment because of a relapse.
“We would see that that would be an example of somebody actually taking an active role in their treatment and getting the help they needed,” said Kolthoff.
The department doesn’t have rules prohibiting any form of medication for opioid addiction, he said, as long as it’s prescribed by a doctor.
“We have people relapse every single day under our supervision. And are they being sent to prison? No. Are they being sent to jail? No,” Kolthoff said.
But Dr. Andrea Weber, an addiction psychiatrist with the University of Iowa, said Beeler’s reluctance to start treatment is not unusual.
“I think a majority of my patients would tell me they wouldn’t necessarily trust going to their [parole officer],” said Weber, assistant director of addiction medicine at the University of Iowa’s Carver College of Medicine. “The punishment is so high. The consequences can be so great.”
Weber finds probation and parole officers have “inconsistent” attitudes toward her patients who are on medication-assisted treatment.
“Treatment providers, especially in our area, are still very much ingrained in an abstinence-only, 12-step mentality, which traditionally has meant no medications,” Weber said. “That perception then invades the entire system.”
Attitudes And Policies Vary Widely
Experts say it’s difficult to draw any comprehensive picture about the availability of medication for opioid addiction in the parole and probation system. The limited amount of research suggests that medication-assisted treatment is significantly underused.
“It’s hard to quantify because there are such a large number of individuals under community supervision in different jurisdictions,” said Michael Gordon, a senior research scientist at the Friends Research Institute, based in Baltimore.
A national survey published in 2013 found that about half of drug courts did not allow methadone or other evidence-based medications used to treat opioid use disorder.
A more recent study of probation and parole agencies in Illinois reported that about a third had regulations preventing the use of medications for opioid use disorder. Researchers found the most common barrier for those on probation or parole “was lack of experience by medical personnel.”
Faye Taxman, a criminology professor at George Mason University, said decisions about how to handle a client’s treatment often boil down to the individual officer’s judgment.
“We have a long way to go,” she said. “Given that these agencies don’t typically have access to medical care for clients, they are often fumbling in terms of trying to think of the best policies and practices.”
Increasingly, there is a push to make opioid addiction treatment available within prisons and jails. In 2016, the Rhode Island Department of Corrections started allowing all three FDA-approved medications for opioid addiction. That led to a dramatic decrease in fatal opioid overdoses among those who had been recently incarcerated.
Massachusetts has taken similar steps. Such efforts have only indirectly affected parole and probation.
“When you are incarcerated in prison or jail, the institution has a constitutional responsibility to provide medical services,” Taxman said. “In community corrections, that same standard does not exist.”
Taxman said agencies may be reluctant to offer these medications because it’s one more thing to monitor. Those under supervision are often left to figure out on their own what’s allowed.
“They don’t want to raise too many issues because their freedom and liberties are attached to the response,” she said.
Richard Hahn, a researcher at New York University’s Marron Institute of Urban Managementwho consults on crime and drug policy, said some agencies are shifting their approach.
“There is a lot of pressure on probation and parole agencies not to violate people just on a dirty urine or for an overdose” said Hahn, who is executive director of the institute’s Crime & Justice Program.
Addiction is considered a disability under the Americans with Disabilities Act, said Sally Friedman, vice president of legal advocacy for the Legal Action Center, a nonprofit law firm based in New York City.
She said disability protections extend to the millions of people on parole or probation. But people under community supervision, Friedman said, often don’t have an attorney who can use this legal argument to advocate for them when they need treatment.
“Prohibiting people with that disability from taking medication that can keep them alive and well violates the ADA,” she said.
This story is part of a partnership between NPR and Kaiser Health News.
While hand-washing is preferred, hand sanitizers with at least a 60% alcohol concentration can be an effective alternative to always using soap and water, but only if your hands are not visibly soiled.
Editor’s note: The World Health Organization has declared that COVID-19, the disease caused by the new coronavirus, has a higher fatality rate than the flu. As of March 4, 2020, nine deaths have been reported in the U.S. Brian Labus, a professor of public health, provides essential safety information for you, from disinfectants to storing food and supplies.
1. What can I do to prevent becoming infected?
When people are sick with a respiratory disease like COVID-19, they cough or sneeze particles into the air. If someone is coughing near you, the virus could easily land on your eyes, nose or mouth. These particles travel only about six feet and fall out of the air rather quickly. However, they do land on surfaces that you touch all the time, such as railings, doorknobs, elevator buttons or subway poles. The average person also touches their face 23 times per hour, and about half of these touches are to the mouth, eyes, and nose, which are the mucosal surfaces that the COVID-19 virus infects.
We public health professionals can’t stress this enough: Proper hand-washing is the best thing you can do to protect yourself from a number of diseases including COVID-19. While hand-washing is preferred, hand sanitizers with at least a 60% alcohol concentration can be an effective alternative to always using soap and water, but only if your hands are not visibly soiled.
The best way to wash your hands.
2. Wouldn’t it be easier just to clean surfaces?
Not really. Public health experts don’t fully understand the role these surfaces play in the transmission of disease, and you could still be infected by a virus that landed directly on you. We also don’t know how long the coronavirus that causes COVID-19 can survive on hard surfaces, although other coronaviruses can survive for up to nine days on hard surfaces like stair railings.
Frequent cleaning could remove the virus if a surface has been contaminated by a sick person, such as when someone in your household is sick. In these situations, it is important to use a disinfectant that is thought to be effective against the COVID-19 virus. Although specific products have not yet been tested against COVID-19 coronavirus, there are many products that are effective against the general family of coronaviruses. Cleaning recommendations using “natural” products like vinegar are popular on social media, but there is no evidence that they are effective against coronavirus.
You also have to use these products properly in accordance with the directions, and that typically means keeping the surface wet with the product for a period of time, often several minutes. Simply wiping the surface down with a product is usually not enough to kill the virus.
In short, it isn’t possible to properly clean every surface you touch throughout your day, so hand-washing is still your best defense against COVID-19.
3. What about wearing masks?
While people have turned to masks as protection against COVID-19, masks often provide nothing more than a false sense of security to the wearer. The masks that were widely available at pharmacies, big-box stores and home improvement stores – until a worried public bought them all – work well at filtering out large particles like dust. The problem is that the particles that carry the COVID-19 virus are small and easily move right through dust masks and surgical masks. These masks may provide some protection to other people if you wear one while you are sick – like coughing into a tissue – but they will do little to protect you from other sick people.
N95 masks, which filter out 95% of the small, virus-containing particles, are worn in health care settings to protect doctors and nurses from exposure to respiratory diseases. These masks provide protection only if they are worn properly. They require special testing to ensure that they provide a seal around your face and that air doesn’t leak in the sides, defeating the purpose of the mask. People wearing the mask also must take special steps when removing the mask to ensure that they are not contaminating themselves with the viral particles that the mask filtered out. If you don’t wear the mask properly, don’t remove it properly or put it in your pocket and reuse it later, even the best mask won’t do you any good.
4. Should I stockpile food and supplies?
As a general preparedness step, you should have a three-day supply of food and water in case of emergencies. This helps protect from disruptions to the water supply or during power outages.
While this is great general preparation advice, it doesn’t help you during a disease outbreak. There is no reason to expect COVID-19 to cause the same damage to our infrastructure that we Americans would see after an earthquake, hurricane or tornado, so you shouldn’t plan for it in the same way. While you don’t want to run out of toilet paper, there is no reason to buy 50 packages.
A Wuhan-type quarantine is extremely unlikely, as a quarantine won’t stop the spread of a disease that has been found all over the world. The types of disruptions that you should plan for are small disruptions in your day-to-day life. You should have a plan in case you or a family member gets sick and you can’t leave the house for a few days. This includes stocking up on basic things you need to take care of yourself, like food and medicines.
If you do get sick, the last thing you are going to want to do is run to the grocery store, where you would expose other people to your illness. You shouldn’t wait until you are out of an important medication before requesting a refill just in case your pharmacy closes for a couple days because all their employees are sick. You also should plan for how to handle issues like temporary school or day care closures. You don’t need to prepare anything extreme; a little common-sense preparation will go a long way to make your life easier if you or your loved ones become sick.
Voters have frequently complained that the debate has been confusing and hard to follow. Here are six things to know as you tune in to the increasingly frenzied primary race.
Health has been a top issue in the presidential campaign during the past year: Not only do the Democratic candidates disagree with President Donald Trump, but they also disagree among themselves.
Voters have frequently complained that the debate has been confusing and hard to follow. Most of the attention so far has been focused on whether the U.S. should transition to a “Medicare for All” program that would guarantee coverage to all U.S. residents — and result in higher taxes for most people. But there is far more to the health debate than that.
The campaign is nearing some key moments — the caucuses in Iowa next week, the New Hampshire primary Feb. 11, voting in Nevada and South Carolina later in the month. By March 3, Super Tuesday, Democrats will have chosen a third of all delegates.
Here are six things to know as you tune in to the increasingly frenzied primary race.
Universal coverage, Medicare for All and single-payer are not all the same thing.
Universal coverage is any method of ensuring that all of a country’s residents have health insurance. Other countries do it in various ways: through public programs, private programs or a combination.
Single-payer is a system in which one entity, usually but not always a government, pays for needed health care services. Single-payer is NOT the same as socialized medicine. The latter generally refers to a system in which the government pays all the bills, owns the health facilities and employs the health professionals who work there. In a single-payer system, such as Medicare in the U.S., the bills are paid by the government but the delivery system remains mostly private.
Medicare for All is a proposal that was originally developed in the late 1980s. Building on the popularity of the Medicare program for senior citizens, the idea was originally to extend that program to the entire population. However, since Medicare’s benefits have fallen behind those of many private insurance plans, the later iterations of Medicare for All would create an entirely new, and very generous, program for all Americans.
Voters are more concerned about health care costs than health care coverage.
While Democrats fight over how best to cover more people with insurance, the majority of Americans already have coverage and are much more worried about the cost. A recent survey of voters in three states with early contests — Iowa, South Carolina and New Hampshire — found voters in all three ranked concerns about high out-of-pocket costs far ahead of concerns about insurance coverage itself.
It’s the prices, stupid.
There’s a good reason voters are so concerned about what they are being asked to pay for medical services. U.S. health spending is dramatically higher than that of other industrialized nations. In 2016 the U.S. spent 25% more per person than the next highest-spending country, Switzerland. Overall U.S. health spending is more than twice the average of other Western nations.
But that’s not because Americans use more health services than citizens of other developed nations do. We just pay more for the services we use. In other words, as the late health economist Uwe Reinhardt once famously quipped in the title of an academic article, “It’s the Prices, Stupid.” A later paper published last year (the original is from 2003) confirmed that is still the case.
Drug companies and insurers aren’t the only ones responsible for high prices.
To listen to many of the candidates’ messages, it may seem drug companies and health insurers are together responsible for most — if not all — of the high health spending in the U.S.
“The giant pharmaceutical and health insurance lobbies have spent billions of dollars over the past decades to ensure that their profits come before the health of the American people,” says Sen. Bernie Sanders on his presidential campaign website. “We must defeat them, together.”
Most insurance spending, though, actually goes for care delivered by doctors and hospitals. And some of their practices are far more gouging to patients than high prices charged by drugmakers or administrative costs added by insurance companies. Wall Street firms that have bought physician groups are helping block a legislative solution to “surprise bills” — the often huge charges faced by patients who inadvertently get care outside their insurance network. And hospitals around the country are being called out by the news media for suing their patients over bills almost no patient can afford.
Democrats and Republicans have very different views on how to fix health care.
To the extent health has been covered in the presidential race, the story has been about disagreements between Democrats: Some want Medicare for All, while others are pushing for less sweeping change, often described as a “public option” that would allow but not require people to purchase a government health plan.
There are much bigger divides between Democrats and Republicans, however. Democrats nearly all support a larger role for government in health care; they just disagree on how much larger it should be. Meanwhile, Republicans generally want to see less government and more market forces brought to bear. The Trump administration has already either implemented or proposed a variety of ways to decrease regulation of private insurance and is weighing whether to allow states to effectively cap their Medicaid program spending.
And in the biggest difference of all for the coming campaign, the Trump administration and a group of GOP-led states are, again, challenging the entire Affordable Care Act in court, arguing that it is unconstitutional based on the 2017 tax law’s zeroing out of the tax penalty for failing to maintain insurance coverage.
The Supreme Court has opted not to decide the case in time for the 2020 election, but it is likely to continue to be a major issue in the campaign.
There are important health issues beyond insurance coverage and costs.
While Medicare for All and drug prices have dominated the political debate during the past year, other critical health issues have received far less attention.
Some candidates have talked about long-term care, which will become a growing need as baby boomers swell the ranks of the “oldest old.” Several have addressed mental health and addiction issues, a continuing public health crisis. And a few have laid out plans for the special needs of Americans in rural areas and those with disabilities.
HealthBent, a regular feature of Kaiser Health News, offers insight and analysis of policies and politics from KHN’s chief Washington correspondent, Julie Rovner, who has covered health care for more than 30 years.
What are the different pressures faced by Anita Hill and Christine Blasey Ford regarding their testimonies of alleged sexual and gender mistreatment by Supreme Court Justices Clarence Thomas and Brett Kavanaugh?
As the founder of the #MeToo movement, why is Tarana Burke, a black woman, getting death threats from black men?
The underlying core of these questions is: What really makes trauma traumatic?
Decades of research on trauma, or physical, sexual or psychological violence, have shown the same thing: Victimization hurts people. Sexual assault in particular can be painful to all who experience it.
However, as a trauma expert who has studied the effect of violence for over a decade, I have found that there is a unique harm for black people and other minorities whose perpetrators are of the same minority group.
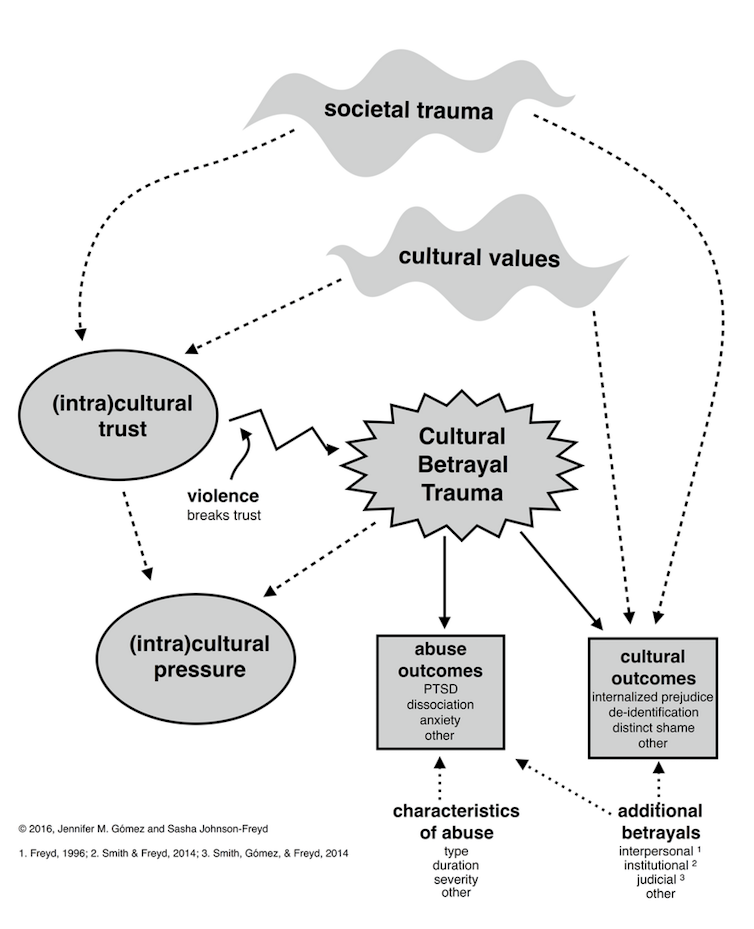
To understand this harm, I created cultural betrayal trauma theory. The general idea of cultural betrayal trauma theory is that some minorities develop what I call “(intra)cultural trust” – love, loyalty, attachment, connection, responsibility and solidarity with each other to protect themselves from a hostile society. Within-group violence, such as a black perpetrator harming a black victim, is a violation of this (intra)cultural trust. This violation is called a cultural betrayal.
The Harms of Cultural Betrayal
Cultural betrayal leads to many different outcomes.CC BY-SA
Cultural betrayal trauma, which is simply within-group violence in minority populations, is associated with many outcomes that go beyond things that are typically studied with trauma, such as post-traumatic stress disorder. It includes some things not often thought about with trauma, such as internalized prejudice – like a black person believing the stereotype that all black people are violent.
(Intra)cultural pressure is another outcome of cultural betrayal trauma. With (intra)cultural pressure, people who experience cultural betrayal trauma are often demanded to protect the perpetrators and the minority group as a whole at all costs, even above their own well-being. With the mandate of “don’t betray your race,” (intra)cultural pressure punishes people who speak out about the cultural betrayal trauma they have endured.
In a recent study, I tested cultural betrayal trauma theory in youth due to the increased risk for trauma and mental health problems in the transition into adulthood.
I surveyed 179 college women online in 2015. Over 50% of these young women were victims of trauma. Just under half experienced psychological violence, 14% endured physical violence, and almost one in three women were victims of sexual violence.
Of the young women who were victimized, over 80% reported at least one form of (intra)cultural pressure. This included their ethnic group suggesting that what happened to them may affect their minority group’s reputation. An example of this could be a black woman who has been raped by a black man being told that she should not go to the police because it will make all black people look bad.
Additionally, I found that controlling for age, ethnicity and interracial trauma, cultural betrayal trauma and (intra)cultural pressure were associated with symptoms of PTSD. Meaning, cultural betrayal in trauma and (intra)cultural pressure were unique contributing factors of mental health problems in ethnic minority college women.
What Does This All Mean?
As I analyzed the findings, I was struck by several things:
The within-group nature of trauma includes a cultural betrayal in minorities that affects mental health.
Trauma gives us only part of the picture.
Group-level responses and cultural norms via intra-cultural pressure impact mental health.
Policy change that combats inequality, such as changes in education, health care, law enforcement and the judicial system, can benefit minorities who experience trauma.
These findings have implications for interventions. Such therapy can address the very real threats of discrimination and the necessity for (intra)cultural pressure. At the same time, these interventions can use (intra)cultural trust to promote positive mental health. Additionally, evidence-informed feminist approaches, such as relational cultural therapy, may benefit people who are exposed to both trauma and societal inequality.
The body of research to date suggests that cultural betrayal may be a unique harm within violence in minority populations, including the black community. As such, the alleged sexual traumas perpetrated by R. Kelly and Clarence Thomas have a cultural betrayal that isn’t found in Woody Allen’s alleged abuse. Moreover, black men’s death threats against Tarana Burke are (intra)cultural pressure that is laced with misogynoir, or sexism in the black community.
Research that incorporates societal inequality can help us understand what makes trauma traumatic. In doing so, our social reactions and therapeutic interventions can ultimately be effective for blacks and other minorities who are exposed to trauma.
I am in favor of a sober revolution in which everyone is comfortable speaking frankly about their struggle with alcohol and other substances.
“I can’t believe how some people will share the most intimate details of their lives on social media. People they don’t even know can see these things. Future employers. It’s shocking.”
I nodded my head in agreement as my biggest client shared her opinion of oversharing the details of your life. We were at dinner with a group, but this was a one on one conversation. I stopped processing what she said after that. My mind raced through the intimate details of my life that I’ve shared with strangers. I’m way beyond Facebook posts when it comes to sharing my struggles with alcohol and how mental illness has impacted my life.
A quick Google search would show my client I’ve written articles, spoken at conferences and on podcasts, and frequently posted about alcohol abuse and mental health issues on my social media. I felt on edge as I drove home that night. Would my client find out I’m an oversharing alcohol abuser? Most importantly, it was the first time I was questioning if it was a good idea for me to attach my name to the issue of alcohol abuse since I wrote my first article on the topic nearly five years ago. Why didn’t I stay anonymous? Was it worth it? Why would anyone choose to make their struggles public?
Why Didn’t I Stay Anonymous?
Five years ago, I made a personal and voluntary choice to write about my struggle with alcohol abuse. I wanted to raise awareness of the role I felt alcohol was playing in my field of design and technology. I had one year of sobriety. I struggled during that year to find a good reference point among my colleagues and friends for what not-drinking looked like. I knew there were others like me. I wanted them to know they weren’t alone. I wanted to put my name and face out as someone they could trust on this issue.
I believe we are more impactful when we remove anonymity from sharing our struggles. People pay attention when an A-list celebrity comes out with their struggle with alcohol or drug abuse. We feel more connected to a disease or condition when someone we know shares with us they have it. In that same way, though not at all a celebrity, I wanted to maximize the impact of sharing my experience. I also thought having others know my desire to stay sober would help hold me accountable in times I craved alcohol.
I had an anonymous childhood. I grew up in a family where one parent had a significant mental illness, and I went through middle school and high school avoiding attention. I reflected on this before I made my alcohol abuse public. I didn’t want to live a life of anonymity when I realized my struggles — both with alcohol and mentally ill family members — are shared by large numbers of people. Perhaps everyone knows someone impacted by one or both of these issues. But we don’t talk about it; not nearly as often as we should. I wanted to contribute to changing that for the better.
I made the commitment to attempt publishing and speaking on the topic of alcohol abuse. I haven’t set the world on fire, but I’ve gained enough traction. I’ve published over a dozen articles and blog posts, videos of conference presentations, and podcasts on this topic. I’ve lived four years with my issues made public.
The Present: Things change – Things Stay the same.
I couldn’t have predicted many of the changes that have occurred since I left anonymity; changes that perhaps would have caused me to reconsider going public.
My works situation has changed. Four years ago, I sat down with one of the partners at the design firm I work for. I told him I’d been sober for a year and I wanted to go public about the need for our industry to do more for those struggling with alcohol issues. I knew my first article on the topic was set for release within 48 hours. I wanted his permission to affiliate myself with the studio in my bio statement. He gave me his full support and that of the other two partners. I knew I wouldn’t lose my job when the article came out.
One year later, a mega-company acquired our studio. A company with many restrictions around communication with the outside world, a company with many restrictions against affiliating yourself with their name. I’ve now worked for this company for over three years. No one at the company from outside of our studio has commented on my alcohol-related writing or speaking.
I’ve done some things to help limit the possibility I’ll get in trouble at work. I’ve shifted how I affiliate myself in my bio: I don’t name my company; I don’t claim any affiliation with my opinion and the company I work for. I post less on social media, as many people from my studio and the larger company follow some of my accounts. I do have anxiety over being asked to remove my writing from public view. I knew this was a possibility if I decided to change employers after going public, but I was surprised to find myself with the same employer but different policies almost overnight
I’m not as concerned about future employers. As I continue to build a foundation of writing and speaking, I’m hopeful to move more towards the space of advocating for awareness of issues related to alcohol abuse as part of my profession. I will choose a future employer based on the support and flexibility they are able to provide me around this goal. And I haven’t given up on exploring the potential for acceptance of my advocacy at my current employer.
My personal life has changed. I was engaged and then married when I first shared my issues with alcohol abuse. I had my wife’s consent to go public. I wasn’t concerned she would judge me; she’d lived through what I was writing about.
I’m now divorced and dating. Potential dates ask for a last name to look me up online prior to meeting and I’m proud of what they will find. I know some might develop negative opinions based on what I’ve written. I’m not concerned about what I might miss, but it’s an example of something I hadn’t considered because my relationship status seemed solid four years ago.
I’m not set on having a sober partner. Almost every woman I’ve had a date with stated they drink. They ask if I mind them drinking on our dates. I don’t. One woman canceled a date after finding out I am sober. She was coming out of a marriage to an alcohol abuser and said she still felt triggered. I respect that. My lack of anonymity allowed us to avoid investing time in something that would not have worked.
Outside of work and relationship changes, I was aware of the potential pitfalls. People know my shit. You can know my flaws before you meet me. I can’t speak for how that might have impacted me. Many people have introduced themselves and congratulated me on staying sober or thanked me for sharing insights they found valuable. No one has ever said to my face they think I’m oversharing or embarrassing myself.
I constantly deal with imposter syndrome, which is when you feel like a fraud for putting yourself forward as someone with expertise. I struggle with this whenever I start writing an article or post meant to help others. I focus on the fact that I’m sharing my experiences in a way I hope helps people. I’m not saying what I’ve done is the only way, or even the best way to get and stay sober. I’m not an imposter as a sober person. No one is. We each do it our own way. If I do something that’s effective for another person then I want to take the opportunity to share that.
What if I do drink? If I relapse or decide I want to become a casual drinker (probably impossible), I will look very hypocritical. I find that helpful in adding to the sense of accountability I have. I know that’s shallow, to care what others think, but I’ve interjected myself into the how to be sober conversation and would deservedly look foolish for failing to hold up my end of the discussion.
A Personal Decision
I can’t speak to whether anyone else should make their sober status public. I am in favor of a sober revolution in which everyone is comfortable speaking frankly about their struggle with alcohol and other substances. Today, we are far from that. I always appreciate when actors, musicians, and sports icons share their struggles. These people have large platforms and can impact society at the change level much quicker than I can.
I believe the benefits of being open about my alcohol issues have outweighed the costs. I’ve been able to play a small part in shaping a message that will need to be repeated through the end of time, it seems: Not everyone drinks. It doesn’t matter why. We need to support those who choose not to drink. We need to support those who are struggling to recognize and treat alcohol abuse, as well as their families. I wouldn’t feel as comfortable entering these conversations if I didn’t have a small body of work to support my experience. I understand most people have no idea who I am or what my background is, but knowing I exist in public forums as a confessed alcohol abuser on a mission to help others with alcohol issues is enough to keep me engaged.
As far as the client from the opening of this piece, I don’t know if they have ever looked me up online or found any of my posts on sobriety. But I have made them aware I’m sober, and they are grateful to have me as the designated driver when we go out for entertainment.
The way of living I have found in sobriety helps me live differently and more beneficially on a day to day basis. This has made for a good life.
I got sober at 29, ten years ago this month. Here are ten ways in which life is drastically different for me now:
1. Every Morning, I Wake Up Clean and Safe
This was not the case for so many years. I have awoken in people’s yards, in stranger’s homes, in cars, with black and blues and broken busted cheeks, with my things stolen or missing, in a jail cell, once in an FBI interrogation office, and countless times in a puddle of my own piss.
2. I’m Never Bored
Seriously, it’s true. For me the notion of getting sober meant a boring life and this was at the top of my list for reasons not to change. But the truth is that I was really bored the last few years I was still using. Bored and exhausted at the same time. In recovery I have learned that my ideas are actually things that can materialize and not just stay mostly conversations on a barstool that might move into reality at a snail’s pace. Today there are not enough hours in the day. I am writing a book, I have a full-time career that’s perfect for me, I see friends daily, I make time for art, I take care of my cats and dog, I have a hundred goals I plan on seeing through. There is no time for withdrawal or hangovers today. I am anything but bored. I am actually alive now.
3. I Prefer This Way of Living
I have some problems and I know what they are: I am impulsive and struggle to think things through, I love chaos and excitement, I live mostly in the past and the future, I am a people pleaser, I obsess about things and about people and I can be really hard on myself. These are all survival skills that helped me in the past somehow but hold me back from reaching my potential. I wish I could say they have changed but they seem to be my autopilot, deeply embedded behaviors. I never graduate my recovery program. The way of living I have found in sobriety helps me live differently and more beneficially on a day to day basis. This has made for a good life.
4. As Long As I Stay sober, I Will Never Have to Be Alone Ever Again
I am surrounded by love and not alone. Before I got sober, I was instead surrounded by people who drank like me. Friends who didn’t drink like me were distant in contact and grew into their own lives understandably. I felt very alone. Not the case anymore. The bonds I have made over time with people in my program of recovery are strong and plentiful. These bonds are strong like those of a cult but I don’t have to give up my dreams, paychecks, and outside contacts. During the darkest times in my sobriety, these people are there. They check up on me as I do them. They want me around on the holidays, want to grieve my losses with me and celebrate my successes. It’s such a gift to know I will never have to feel alone again if I stay sober. And if I don’t stay sober, which of course is always a possibility, they will undoubtedly help me if I want to get sober again.
5. I Am Well Aware That Alcohol and Drugs Will Not Make It Better
Without them it turned out I was pretty sick. At two years sober I was controlled by relentless anxiety and fear. Now I understand my trauma reactions and why I was abusing substances the way I was. Without numbing out my thoughts raced all of the time, my Obsessive Compulsive Disorder which I struggled with much of my life got so much worse and I started to try and obsessively “fix” people and situations for which in reality I had minimal control over. My body ached from being on high alert constantly. At ten years sober I am aware that when my outside world is stressed and overwhelmed, my warped stress response system goes into survival mode trying desperately to make sense of things by detective work, compulsive checking and seeking out ways to feel safe. Alcohol and drugs used to calm my system and was helpful until it started being more harmful than helpful. Now when I am caught up in my stress response system, I have learned how to ease it without abusing substances. and sometimes I just have to hang on, knowing it will pass.
6. I Realize I’m Intelligent and Very Capable
Much of my life I was considered to have learning disabilities and was even voted “most clueless” in my high school yearbook, yes, I still remember that bull&8%#- class of 1999. Through all the testing over the years I received for learning problems no one ever asked about what life was like at home. Due to early childhood loss and trauma my amygdala was working on overdrive and controlled by fear as I was worried all the time that something bad was going to happen to one of my family members or to me. This makes concentrating in a classroom setting pretty impossible. Today I have graduated college with honors, hold a Master’s degree and subsequent license and I am an expert in my specific field. Go figure.
7. I Now Have Help from Hundreds of Higher Powers That Do Not Screw Me Over Like Using Did
The whole concept of the Higher Power thing annoyed and angered me prior to sobriety. I wasn’t against there being some meaning to the universe, but I did not respect some of the older recovery literature and signage in 12 step meetings which I thought assumed the higher power was “God” and was male. Luckily, I found many recovery type meetings which welcomed a much expanded and evolved idea of what a Higher Power is. Today a few of the powers outside of myself that I rely on to stay sane, sober and grounded include but are not limited to; the making of calls to people in recovery, using guided meditations, laughing with friends, water; swimming or taking baths, daily meditative readings, using materials to make art or appreciating art someone else has made, exploration and belief in some spiritual theories, healthy eating, paying attention to synchronicities and to my breathing. You could say I am living a more spiritual life and, yes, I am okay with saying that now.
8. With a Clearer, Open Mind, I Understand That for There to Be Joy, There Must Also Be Painful Experiences
One cannot exist without the other. If there were only joy, it would be the status quo, and we could not appreciate it as joy, it would just be the way things are- the typical. For example, when you finally get to enjoy a piece of toast after getting over the flu, isn’t it just a great treat? I do not regret my past, or my pain. It has given me the life I have now, which is often a great treat. When I am in pain, I try to remember there is an opportunity for greater joy. Not always easy of course at the moment. But in time with reflection it’s clear that the universe has always led me to better things if I let it and trusted the process.
9. I Know That Sometimes My Worst Fears Will Come True, and That’s Okay
I do not need to use; throw away my sobriety to escape the pain. I wrote out a list of my fears when I was about a year sober. There were over 300. Many of them have come true; family and friends have died, I have been heartbroken, I have become ill at points, I have been judged and criticized. I have spent so much time in my living in fear. I have managed to not use to ease the bouts of fear, which is what I did for so long. I know using will only lead to more and more pain. I ease it now with a variety of other things such as cognitive behavioral techniques, meditation, talking to others in recovery, looking back on the times things were so hard I didn’t think I would make it through and I did make it through.
10. I Love Myself No Matter What
More and more all of the time. I was not able to show myself love for a very long time. I didn’t realize that until I was sober for a good while; really, for years. This has been a great gift of recovery. I am not always perfect at finding complete love for myself, but daily I can tune into it more easily. This self-love has dramatically changed my life and my ability to take risks, forgive myself, let go of shame and leave toxic situations. I have to see myself as my own daughter and protect her. This love is really what keeps me sober these days one day at a time.
A North Carolina rehab program promised recovery, free of charge, to people struggling with drug addiction. When they arrived, they were put to work without pay at adult care homes for the elderly and disabled.
Jennifer Warren has spent years recruiting the poor and desperate to her drug rehabilitation program in the mountains outside Asheville, North Carolina.
She promised them counseling and recovery for free. When they arrived, she put them to work 16 hours a day for no pay at adult care homes for the elderly and disabled.
Thrust into the homes with little training or sleep, the rehab participants changed diapers, bathed patients and sometimes dispensed the same prescription drugs that sent them spiraling into addiction in the first place.
For some, the temptation proved too great. They snorted prescription pain pills, swallowed droplets of morphine from used medical syringes and peeled fentanyl pain patches off patients and sucked them to get high.
Then there were the allegations of assault. At least seven participants from Warren’s program, Recovery Connections Community, have been accused of sexual misconduct or assault of patients at the homes. Former participants and workers said no one reported the incidents to social services, as required by law. The accused continued working or were simply transferred to another care home.
“There’s a whole lot in the program that’s covered up,” said Charles Polk, who completed Warren’s program in 2017 for alcohol addiction. “The only thing she thinks about is the money.”
Charles Polk of Monroe, N.C., completed the Recovery Connections program last year. He says the program’s director, Jennifer Warren, thinks only about money. Credit: James Nix for Reveal
Amid a nationwide opioid epidemic, treatment remains out of grasp for most people struggling with addiction. Those with wealth and insurance often are able to pay thousands of dollars for private long-term programs. But the less fortunate have become easy prey for rehabs with a tantalizing promise: freedom from addiction for free.
To pay for their stay, participants must work full-time jobs and surrender their pay. An ongoing investigation by Reveal from The Center for Investigative Reporting has found that many programs exploit this arrangement, providing few actual services while turning participants into indentured servants.
In North Carolina, Warren has turned her nonprofit rehabilitation program into her personal empire. She worked the people in her program to exhaustion, while regularly vacationing in places such as Paris, Greece and New Orleans for Mardi Gras, according to former participants and state records. She diverted nonprofit donations meant for the program – appointments at beauty salons and concert tickets – to herself and used participants’ food stamps to stock her own kitchen.
In addition to working at adult care homes, the 40 or so men and women in Warren’s program have baby-sat her children, cared for hundreds of her exotic pets and cleaned her house.
“It’s like slavery,” said Denise Cool, who was addicted to crack cocaine when a judge ordered her to the rehab in 2011, “like we were on the plantation.”
Jennifer Warren is shown in a 2015 booking photo after she was caught illegally collecting thousands of dollars’ worth of food stamps. Credit: Buncombe County Bureau of Identification
Even after being stripped of her counseling license in 2012, Warren continued to operate her program with impunity. Authorities from four separate state agencies neglected complaints, botched investigations and stood by for years as Warren flouted rules they were supposed to enforce.
It was not until Reveal questioned state officials about their inaction that they began taking steps to curb the abuses.
Warren, who is 52 years old, declined to answer questions from Reveal.
“I have no reason to believe that you will report anything positive about our program or are interested in the people’s success stories, of which there are many,” Warren wrote in an email.
When confronted by a former participant in a private Facebook message in February, Warren responded, “It’s so easy to buy into the negativity.”
“Because of the structure of this kind of program, many people leave with resentments and are disgruntled,” she wrote in the message, obtained by Reveal. “I have spent the majority of my adult life trying to give back.”
Founded in 2011, Recovery Connections Community has grown to include three locations, run from rural homes near Asheville and Raleigh.
Hundreds of people have sought help from Recovery Connections over the years. Many are sent there by the courts as an alternative to prison. Others come directly from hospitals, mental health facilities and state-funded detox centers.
Whitney Richardson was addicted to heroin and facing prison time for burglary when a North Carolina judge ordered her to complete the two-year program in 2014 as part of a plea agreement.
Judges and probation officers weren’t supposed to use unlicensed rehabs such as Recovery Connections for treatment. And the rehab specifically had been on probation officials’ radar. In internal emails, one official said it was “a bad agency and is run by dangerous people.”
Richardson fled four months later. She was so scarred by the experience that she vowed never to attend rehab again. When she later relapsed, she said she got herself clean by buying Suboxone on the street.
“It’s not right to take advantage and subject people to abuse like that when they’re trying to better their lives,” Richardson said. “No one should ever go to that place.”
***
Jennifer Warren – known then as Jennifer Hollowell – was working on a doctorate at the University of Alabama when she got hooked on crack cocaine.
She dropped out of her clinical psychology program and at 27 years old checked herself into a residential rehab program in Winston-Salem that required that she and other participants work for free.
Warren flourished in the rehab, becoming the director’s assistant once she graduated. “I wanted to be like her, and she became my role model,” she would later recall.
But in 2002, after the director left amid allegations that she had stolen money and – former employees said – dated a client, Warren and several other clients decided to start a program of their own. They called it Recovery Ventures.
With her flowing blond hair and colorful dresses, Warren projected the image of a free spirit. She described clients as family and would invite them to socialize in her home, which was adorned with fairy figurines and painted bright purple inside.
“She could just look at you and just read straight through you, I swear to God,” said former client Lakindra Edwards. “Like, wow. She don’t even know me, but she told me everything about me.”
But Warren soon began to cross ethical lines. She instructed her clients to clean her home and care for her growing collection of llamas, miniature ponies and exotic birds. Then she, too, began a romantic relationship in 2008 with a client she was counseling.
Phillip Warren would spend the night at her house, and they would kiss around other clients. Dating a participant violated a host of state ethics rules, but when friends and colleagues tried to intervene, Jennifer Warren crumpled into tears.
Undeterred, she moved up Phillip Warren’s graduation date and moved him into her house. The two married years later.
By 2011, multiple complaints about Jennifer Warren had reached the North Carolina professional licensing board. In the official document later filed against her, the board chastised her for her ethical breaches and said she wasn’t cut out for the rehab business. In fact, the more time patients spent around her, the licensing board wrote, the more likely they were to relapse.
Warren “used and exploited her clients for her personal benefit” and “failed to maintain appropriate boundaries between herself and her clients,” the board wrote. The state eventually revoked her counseling license.
The rehab fired her in 2011. A few days later, Warren struck out on her own, founding Recovery Connections. To pay for her program, she turned to a handful of employers always in need of workers: adult care homes.
***
Rachel Thomas was working one night in 2016 at Candler Living Center, a home near Asheville for mentally ill and disabled adults, when a worker from Jennifer Warren’s program came sprinting down the hall.
An elderly resident was gasping for air and repeatedly vomiting. Thomas discovered that the rehab worker – who was not trained to dispense prescription drugs – had given the patient the wrong medication.
“He actually about killed one of the residents,” said Thomas, who no longer works at Candler. “He had no idea what was going on.”
A former employee at Candler Living Center, a facility for mentally ill and disabled adults outside Asheville, N.C., contracted with Recovery Connections for workers. It houses nearly 30 residents. CREDIT: NANCY PIERCE FOR REVEAL
Participants from Recovery Connections worked in at least nine homes over the years. Some worked as janitors and cooks, but the majority worked as personal care aides.
In North Carolina, personal care aides must receive at least 80 hours of training, during which they learn how to safely feed, lift and bathe patients. But many rehab workers interviewed by Reveal said they never received the training required by law. Some Recovery Connections participants also dispensed medication with no training, even though state law requires a special certification.
“I would die if someone like that was taking care of my mom,” said Renee Thayer, a former program participant who was assigned to work as a personal care aide in 2012.
The rehab workers cost the facilities less than regular employees. Some homes paid Recovery Connections the minimum wage – $7.25 an hour – for each worker and did not pay workers’ compensation, insurance or overtime, according to former managers and internal records obtained by Reveal.
Disasters Happened All the Time
One employee at Hominy Valley Retirement Center would unlock the medicine cart and place pain pills into white paper cups. Then, rather than take the prescription drugs to the residents herself, she would order the rehab workers to pass out the pills while she slept on a recliner, said Charles Polk, a former participant who also dispensed the drugs.
“Lots of people relapsed and got high that way,” he said. “They stole the meds. They would just take it.”
Fentanyl pain patches, which slowly release an opioid up to 50 times more powerful than heroin, were in particularly high demand. When it was time to shower patients in chronic pain, some rehab workers would peel off the patches and keep them for themselves.
“They would take their patches off them and suck the fentanyl out,” said Ian Hays, a former manager at Recovery Connections. “One girl told me, ‘I got high every day in the fucking program.’ ”
***HELP US REPORT THIS STORY We’re trying to figure out how many work-based rehabs there are in the United States. Fill out this form if you know about one. And email us if you’re a journalist or news organization that wants to report on rehabs near you.***
At least seven rehab workers have been accused of sexual assault or misconduct with patients at the homes. Former employees said none of the allegations were reported to authorities, as required by law. Reveal could find no mention of any of the alleged assaults in thousands of pages of police reports, Adult Protective Services records and county and state inspections. The accused continued working or simply were transferred to other facilities.
One male rehab worker was accused of sexually assaulting a disabled elderly woman in the shower at Candler in 2016. After the incident, the woman refused to let the rehab worker shower her.
“I don’t want him to do it!” she cried while pointing at the worker, recalled Polk, who witnessed the interaction.
In response, Candler barred male rehab workers from bathing female residents, according to seven current and former employees and participants. As of mid-May (2018), the man still was working at the home.
Chris Damiani, chief executive officer of the company that owns Candler and Hominy Valley, said his agency had never had problems with rehab workers. He said that none of the alleged assaults were reported to management and that his company was investigating the issues raised by Reveal’s reporting.
“We do not take any report of abuse, neglect, assault, theft or drug use lightly,” Damiani said.
Cedarbrook Residential Center, an assisted-living facility in Nebo, N.C., houses 80 residents and used workers from Recovery Connections Community. Credit: Nancy Pierce for Reveal
In 2014, another rehab worker was accused of sexually assaulting a disabled woman in her bedroom at Cedarbrook Residential Center, the woman and four former employees said.
She said she fought him off and immediately reported the incident, but the administrator “plumb out ignored me.”
“I hated the place,” said the woman, who left the facility in 2016. “I felt like I was literally in hell.”
Frederic Leonard, Cedarbrook’s owner, said the facility never filed a formal report with the county Department of Social Services because the facility conducted its own investigation and concluded that an assault had not occurred. He declined to provide more details about the internal investigation.
“We have safeguards in place to prevent misconduct of this type,” he said. “It is difficult when mentally ill adults, who are suffering from severe mental illness, are also poor historians of fact.”
The accused worker continued to work at the facility for several days. His presence terrified the patient who had accused him, she and a former employee said.
At Recovery Connections, Warren dealt with the alleged assault in her weekly therapy group. Rather than call police, she placed the man in the middle of a circle while his peers screamed at him and called him a sexual predator, according to two former participants.
“They all went off on him,” said Blake Loving, who attended the therapy session. “He just sat there.”
After the session, Warren sent the accused worker to another care home.
“It was really sick,” said Whitney Richardson, who also attended. “They just kind of wanted to brush it under the rug.”
***
Jennifer Warren collects a salary of about $65,000 a year, according to tax filings, but that money alone never seemed to be enough. For years, she has used her rehab’s nonprofit status as a vehicle for personal enrichment.
Every day, a group of Warren’s clients said they were expected to make hundreds of phone calls to businesses and major corporations asking them to donate goods and services, according to state records, former participants and staff. They asked Tommy Hilfiger for designer clothes, Hilton for hotel stays and The Cheesecake Factory for free meals. Warren used the nonprofit to score free concert tickets to see her favorite bands.
Jennifer Warren’s Trips
The donations were tax deductible and were supposed to go to program participants. But Warren got first pick of everything.
“Jennifer and them got all the good stuff,” said Jessica Stanley, who attended the rehab in 2016 and called businesses on the program’s behalf. “It was a little hustle-scam.”
Participants routinely called nail and hair salons to book free appointments. They said the salon visits would help rehab participants “build their self-esteem.” But Warren was the one who showed up.
“She was taking advantage of all the donated manicures and pedicures,” said Ian Hays, the former Recovery Connections manager. “She used to go to one place in the mall all the time.”
During one appointment, a hairstylist asked Warren how long she had been in the program, according to a former staff member who witnessed the interaction and records from a state investigation. When Warren admitted she was the founder, the stylist was livid.
Warren also ordered program participants to sign up for food stamps, which former participants said she used to stock her own kitchen.
In 2015, Warren pleaded guilty to financial assistance fraud for lying about her income and illegally collecting thousands of dollars’ worth of food stamps. She was sentenced to 45 days of probation. But participants say she continued to use their benefits to fill her personal pantry.
While Warren got steaks, participants said they often were left with little more than Hamburger Helper, crackers and tubs of peanut butter. At times, they complained there was no food at all.
“Sometimes we ate ramen noodles at night,” recalled Roshawnda McIllwain, a former participant who left the program last year. “Some days, I went hungry.”
But there was always money for animals.
Warren spent more than $32,000 in program funds on animal expenses, according to the nonprofit’s tax filings from 2014 and 2015.
She bought goats and sheep at animal auctions around the country. She had two arctic foxes, large ostrich-like birds called rheas and sugar gliders – small marsupials that resemble flying squirrels. Warren claimed they were for the rehab’s animal therapy program.
“Some people collect stamps. Some people collect shoes. Jennifer’s got a thing for collecting animals,” said Hays, the former manager.
Warren keeps dozens of them at her home in Black Mountain, participants said. Her bedroom is stacked with cages of toucans and other tropical birds.
At one of Recovery Connections’ outposts near Raleigh, an entire barn is crammed with animals, according to participants. Guinea pigs tumble over each other in crates. Rats multiply by the dozens. Inside a dimly lit garage, monkeys languish in cramped cages. Several participants recalled burying dead llamas in the program’s yard.
Even though the program had horses for its “equine therapy program,” participants said they weren’t allowed to ride them.
Julia Harris said she was struck with one thought when she checked herself into the program in 2017.
“I have landed in an insane asylum,” she remembers thinking. “I’m in a filthy house with animals and animal fur. And this is supposed to be a rehab?”
Julia Harris, pictured at her home near Brevard, N.C., said she was struck with one thought when she arrived at Recovery Connections last year for help with an alcohol problem: “I have landed in an insane asylum.” Credit: James Nix for Reveal
***
For some people, the worst part of Jennifer Warren’s program was not the work at the care homes or the personal chores – it was the therapy groups.
The sessions usually occurred at Warren’s house. The group sat in a large circle of folding chairs and loveseats while each person took a turn in “the hot seat” in the middle. The other patients then cursed, screamed and hurled insults at the person for up to 45 minutes at a time.
Spoiled brat.
Stupid bitch.
Motherfucking whore.
Participation was mandatory. People frequently broke down crying. Some participants said Warren and others seemed to relish it.
“You see certain people planning this shit all week, looking for stuff to use against you,” said Scott Hucks, who left the program in 2016. “It’s like a joke, it’s like a game. Just entertainment.”
Sometimes, Warren would black out the windows and keep a select group awake for days on end as they recited their life stories. If anyone started to doze off, participants said they were sprayed with water. Some people said they began to hallucinate.
“It’s like CIA torture,” said Heather Fox, who left the program last year.
Warren said the groups were meant to teach participants conflict resolution skills. They learned how to confront the harshest realities of their lives and move past it, she explained in a deposition for a 2010 lawsuit brought by a client who found her first rehab, Recovery Ventures, abusive.
“I wouldn’t say it’s verbal abuse,” she said. “It’s an incredible healing opportunity.”
“Is there screaming involved?” the lawyer asked her.
“Sometimes,” Warren replied.
Warren’s therapeutic tactics are rooted in a drug rehab program called Synanon, which was founded in 1958. Studies have shown that the group sessions, which involve screaming and insults, can be catastrophic for people with poor mental health and low self-esteem. Law enforcement officials later denounced the program as a cult.
Most participants interviewed by Reveal said they found Warren’s therapy sessions humiliating. Those who complained were punished with more work. They were forced to scrub floors with a toothbrush or cut grass with a pair of scissors.
“They wanted us to be so broken down emotionally that we would listen to whatever they said,” said Heather Teatzner-Brown, who attended the rehab for alcohol addiction and fled in the middle of the night in 2016. “Just take it and not have an opinion or your own mind.”
Some former participants interviewed by Reveal spoke positively about the program, saying Warren and her rehab were there for them when no one else was.
“If you’re at a crossroads in your life and you’ve burned up every bridge out there, it’s the best way,” said Rick Taylor, who graduated in 2014 and credits it with helping him overcome a drug addiction. “All I had to do was just surrender and do what I was told.”
Others left the program worse off than when they arrived. Some turned to drugs to cope. Many participants told Reveal that they fled into the mountains, sometimes in the rain or snow or in the middle of the night.
“I was physically sober, but my mind was way worse than it ever was before when I was using,” recalled Tommy Farwick, who attended the program in 2012. “I had zero desire to live anymore. I just wanted to die.”
Through all this, Warren demanded that people work around the clock because the more they worked, the more money they brought in for the rehab.
“Y’all need to make some money,” Hays recalled her saying.
***
North Carolina regulators were well aware of the abuse at Recovery Connections.
Soon after Jennifer Warren opened in 2011, the Department of Health and Human Services received a complaint alleging that she was operating an unlicensed rehab program, in violation of state law. In North Carolina, any facility offering 24-hour treatment is required to be licensed.
When investigator Joy Allison arrived at Recovery Connections to check it out, Warren greeted her warmly. Even though Warren was advertising her program as “substance abuse treatment” online and in brochures, she told Allison a different story: She was running halfway houses, not a treatment program.
Allison accepted that explanation and then offered Warren a tip: If she said she was operating a “12-step, self-help” program, Warren could avoid state oversight completely. Warren used the new language on promotional materials but changed little else.
Seven years later, that decision continues to allow Warren to operate her rehab free of government oversight. But the complaints haven’t stopped: forced labor, self-dealing and abuse.
Each time, Allison gave the same answer. “I have continued to receive calls/complaints about this program but, have explained that they are exempt from licensure,” she wrote in an internal email in 2016.
After questions from Reveal, the state health department finally began to crack down.
On May 16th 2018 it banned Recovery Connections from sending participants to work as caregivers at adult care homes, potentially cutting off the program’s main source of funding. The department said Recovery Connections must be licensed as a staffing agency to continue dispatching workers.
But the department said the program still is not required to be licensed as a drug rehab center.
Recovery Connections has escaped accountability from other state agencies as well.
Since 2011, the North Carolina secretary of state’s office has received complaints that Warren has pocketed donations meant for the program. Its investigators conducted a full investigation, speaking with business owners who had been defrauded by Warren and reviewing internal call logs and financial documents.
But the agency ultimately dropped the case. Its reason: Participants never sent officials signed and notarized affidavits.
Recovery Connections got to keep its charitable solicitation license and nonprofit status, which allows Warren to continue to collect tax-deductible donations from businesses and the public.
In exasperated emails to authorities, the directors of several licensed rehab centers expressed their dismay that Warren kept dodging accountability.
“This individual believes that the rules do not apply to her, no matter how many warnings or disciplinary actions are taken,” David Martin, who had co-founded Warren’s first rehab with her, wrote to the attorney general’s office in a July 2012 email.
Martin ticked off her latest transgression. Warren “spent the entire month of June at the beach” and used the rehab’s food stamps for herself, he wrote. Was this something the attorney general would pursue?
An investigator promised to look into it, but nothing came of it.
The North Carolina Department of Public Safety had its turn to crack down around the same time. Probation officers began hearing complaints in 2012 from people who had been ordered by the court to go to Recovery Connections.
In internal emails, probation officials agreed that the program was unsuitable for offenders and griped about Warren’s sordid history. But they continued to allow probationers to attend.
“We are not responsible for policing the agencies available to the offenders,” one administrator wrote in an internal email.
Following questions from Reveal, probation officials finally took action against the rehab.
“We have determined that the Recovery Connections locations do not align with our mission, vision, or goals,” the department wrote in a May 8 memo (2018). Going forward, no probationer will be allowed there.
But hospitals and short-term treatment centers continue to send people to the program. So do social workers at state-funded detox and psychiatric facilities. Recovery Connections is always willing to accept those who have nowhere else to go.
Jennifer Warren is waiting for them.
More from the All Work. No Pay. series Read: Impact: Officials take action on rehab work camp in response to Reveal investigation Read: They thought they were going to rehab. They ended up in chicken plants Read: Inside a judge’s rehab: Unpaid work at a local Coca-Cola plant Read: Response to work camp investigation: ‘Nothing short of slavery’
When I was in a 12-step program, I had so much shame… Some people seemed pissed off when you relapsed. I get that it’s upsetting, but have a little compassion.
Erin Khar is an award-winning writer known for her deeply personal essays on addiction, recovery, mental health, parenting and self-care. “Ask Erin,” her weekly Ravishly column, attracts more than 500K unique readers per month. Her work is published in SELF, Marie Claire, Redbook, and anthologies including Lilly Dancyger’s Burn It Down: Women Writing About Anger. Her first full-length memoir, Strung Out: One Last Hit and Other Lies That Nearly Killed Me (Park Row Books, February 25), will be released this month.
Khar battled heroin for 15 years. Her intro to opioids came in pill form at age eight. It was the year her parents split up. In Strung Out she writes, “My Dad had moved out and my mother drifted from room to room in our old Spanish house with a weightlessness that I could tell threatened to take her away.”
Khar suffered from overwhelming feelings that she didn’t understand. “A panic spread across my chest, filling my body with heat, trapping me. I ran to the bathroom and locked the door. As I reminded myself to breathe, some instinct led me to the medicine cabinet.”
With anxiety pounding, the third grader fumbled past Band-Aids and Tylenol and found her grandmother’s bottle of Darvocet, which warned: “May Cause Drowsiness and Dizziness.” She wanted so badly to stop hurting she popped two big red pills into her mouth, then gulped from the faucet to wash them down. The burning heat of anxiety soon gave way to a “lightness of little bubbles.” Erin felt like she might float out of her body; this was the escape she’d yearned for.
Strung Out depicts one person’s journey against the backdrop of America’s opioid crisis. The book is written in gorgeous, accessible prose. Candor and vulnerability come through in a natural, believable voice, conveying what many trauma survivors know intimately: pain, anxiety, rage, depression.
Khar snorted heroin for the first time at age 13. At first, she’d said no to the boyfriend urging her to try it; her stolen pills felt like enough. But her guy persisted, describing it as a much better high. It was also the quickest route to forgetting. When Khar was four, a teen boy began molesting her. The abuse continued for years. Like many survivors, Khar told no one and desperately tried to block it from her mind.
“I needed to be somewhere else, someone else,” Khar told The Fix.
Strung Out is a page-turner that follows the progression of addiction: Narcotics seem like a magical solution until the relief morphs into a monster roaring for more. Opioids are now responsible for 47,000 deaths per year—that’s nearly two-thirds of all drug-related deaths in the U.S.
Reading Khar’s book felt like listening to a confidante, a kindred spirit who “got me.” We sat down in a New York City garden to talk about the hell of addiction and colossal relief of long-term recovery.
What idea sparked this book?
I wrote Strung Out because it was the book I wish I’d had when I was younger. I want to open up the conversation. Why do people take drugs? And why can’t they stop? The more we talk about it the more we can get rid of the stigma and shame surrounding it. Many people still don’t seem to understand addiction. I want to encourage empathy and compassion and give people hope.
I love that your then 12-year-old son asked if you ever did drugs. Can you tell me about that?
At first, I pretended I didn’t hear him. [Laughs] I tried not to cringe at my deflection.
I stalled by saying, “That’s a complicated question.” I didn’t know what to say. I did use drugs. A lot of them. Heroin was on and off from 13 to 28. That’s when I got pregnant with him. But how much should I tell him? I’d smoked crack, done acid, taken Ecstasy.
You describe childhood guilt and shame vividly. Looking back, do you think that was rage turned inward?
Oh yeah. It definitely had to do with early trauma. All I knew then was a nagging feeling. It wasn’t until I was 19 that I came to terms with everything. Before that, I minimized what happened to me, trying to shove [memories] aside. It took a long time for me to see that my therapist was right: my anger had sublimated into guilt.
Do you look back now and understand your feelings of shame?
Yes. I took responsibility for things because it gave me the feeling that I was in control. Can anyone process that kind of childhood trauma all in one go? I don’t know. Maybe it takes a lifetime to process? Maybe I’m still processing it.
Yes. Even though I’ve done a lot of work on myself, I still have hypervigilance. My body reacts strongly to some situations, like if I’m startled by something, and especially if I’m asleep.
Can you describe things that helped? Especially for anyone who is trying but can’t stop using.
The first thing was accepting that I wasn’t going to be fixed overnight. Then it was forgiving myself for relapsing constantly. For me, whatever I’m dealing with, if I break it down into small, digestible increments, it’s a lot easier to handle. Focusing on the big picture is not helpful. That’s why they say a day at a time.
How did you stop relapsing?
By being honest about relapses. When I was in a 12-step program, I had so much shame. It was detrimental to worry about being judged at meetings. [Some] people in AA seemed pissed off when you relapsed. I get that it’s upsetting but have a little fucking compassion. [So] I hid relapses, which made it a lot easier to do it again. Finally, I was honest about [chronically] relapsing and that helped me stop. You do not have to relapse. It’s not a requirement of recovery but I don’t think that we unlearn things in 30 days or 60 days or 90 days or a year. I don’t think it happens that quickly. For anyone who struggles with addiction, we want immediate relief.
Like pushing a button?
Yes. I wanted to be numb. Stop thinking. In recovery, my biggest life lessons were learning to have patience, be honest, and work on accepting things I have no control over.
Did you find things easier when you began opening up?
First, I had to get through my fear that people were always judging me. It took work. I wouldn’t say it was easy but yes, I did get better.
How do you feel about your upbringing now?
I definitely don’t blame my parents for any of the choices I made. Even the choices when I was really young. I hid the sexual abuse and my depression from them. I hid my suicidal feelings. If my parents had stayed together and everything had been perfect, I may still have hid things. It may be a function of my personality.
Today I have a really good relationship with both of my parents and they have a really good friendship with each other. I will forever be grateful that no matter what happened, through everything I did, they never turned their backs on me. I have a very different idea about tough love than I used to. When I was first trying to get sober, the general idea of interventions and dealing with somebody who was addicted was this hard line of tough love.
I used to deal with people that way. But now, I really don’t think it works. That doesn’t mean that you should enable people. But, for me, I was lucky. Despite everything I had done to my parents—years of lying and stealing—our family connection remained. That door was still open when I finally asked for help.
The “lonely cell,” as she called it, broke her in less than a day. She apologized. She told deputies she’d learned her lesson. More importantly, Taylor said, “I was just being quiet.”
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for The Big Story newsletter to receive stories like this one in your inbox.
BAKERSFIELD, Calif. — Shackled at the wrists and ankles, Christine Taylor followed a red line on the basement floor directing her to the elevator at Kern County’s central jail. She heard groans and cries from among the hundred people locked above, a wail echoing through the shaft.
It was minutes before daybreak on a Monday morning in May 2017 as the elevator lifted her toward the voices. Jail staff had assigned Taylor to something called “suicide watch,” a block of single cells where she’d be alone 24 hours a day. The sound of other people would soon become a luxury.
What a stupid mistake, Taylor fumed.
Earlier, she had argued with jail staff during her booking at the downtown jail. Have you ever attempted suicide, a deputy asked. Taylor glared back, her hands trembling. She had never been in serious trouble with law enforcement, and she considered her arrest that night a gross misunderstanding.
“Do you think I’m going to try to kill myself with my shirt?” Taylor responded, flippantly. “Maybe.”
Her answer got her a glimpse of how the jail handles people it perceives as suicide risks.
Within minutes, deputies moved Taylor into a changing room on the third floor and had her strip naked. They handed her just two items: paper-thin clothes that come apart under pressure and a blue yoga mat.
Exhausted and scared, she followed orders, walked down a hall and stepped into a bathroom-sized isolation cell. The door slammed behind her. The floors felt colder inside, and a mold smell came up from the toilet-sink fixture. A bed was mounted to the brick wall. Hazy fluorescent lights reflected off the ash-white paint. And, as Taylor soon learned, jail staff never turned them off.
To shield herself, she crawled under the bed and put the yoga mat over her torso like a blanket.
She pressed her eyelids shut but couldn’t block the glare or the rush of tears.
“Cruel and Unusual” Punishment; No Limits
Each year, the Kern County Sheriff’s Office sends hundreds of people into this kind of suicide watch isolation. Inmates awaiting trial spend weeks and sometimes months in solitary, according to state and county records. When those cells fill up, deputies place people into “overflow” areas, rooms with nothing more than four rubberized walls and a grate in the floor for bodily fluids. They receive no mental health treatment, only a yoga mat to rest on.
Kern County sheriff’s officials say they turned to isolation rooms to help prevent deaths after a spate of jail suicides that started in 2011.
This wasn’t what state lawmakers envisioned when they undertook a sweeping criminal justice overhaul nearly a decade ago to alleviate what the U.S. Supreme Court deemed the “cruel and unusual” conditions for people in overcrowded state prisons. Those prisoners, the court found, would languish for months, even years, in “telephone-booth-sized cages” without treatment, resulting in “needless suffering and death.”
California’s reforms, dubbed “realignment,” diverted thousands of offenders to county jails so, among other things, the corrections system could see to basic health needs and meet minimum constitutional requirements. That shift also transferred billions of dollars to local sheriffs to better run jails.
Some, like Kern County Sheriff Donny Youngblood, have rejected warnings from the state to improve the outdated and often brutal forms of isolation that helped trigger the state’s prison crisis.
The state can’t do much about it, a McClatchy and ProPublica investigation found. The California Board of State and Community Corrections, which is supposed to maintain minimum jail standards and inspect local facilities, has no legal authority to force local lockups to meet those standards or ensure inmates are physically safe and mentally sound.
Last year, for instance, a state board inspector called out the Kern County Sheriff’s Office for 27 violations, a majority of them for using yoga mats instead of mattresses in suicide watch cells. But his letter read more like an invitation than a warning. “If you choose to address the noncompliant issues,” he wrote, “please provide your corrective plan to the BSCC for documentation in your inspection file.”
The sheriff’s office disregarded the findings and bought more than 100 additional mats this year, agency records show.
“It’s completely unethical, and counter to clinical evidence for what people need,” Homer Venters, the former chief medical officer of New York City jails, said of Kern County’s suicide watch. “For any human, that represents punishment and humiliation.”
Isolation practices save lives, Kern County officials argue. But records show the strategy didn’t work; inmates continued to kill themselves.
In one case, an inmate hanged himself in a suicide watch cell, after grabbing an extension cord that guards left within reach. Since 2011, 11 others have taken their lives in other parts of the jail. During the past four years, Kern County had the highest suicide rate of the state’s 10 largest jail systems, with 5.61 deaths per 100,000 bookings, close to twice the statewide rate, an analysis by ProPublica and McClatchy found. Overall, inmate suicides declined slightly in California county jails over that period.
The state’s board has no authority to investigate deaths in local lockups. The agency answers to the Legislature, which has not held a single hearing about jail inspections or the dozens of gruesome deaths in facilities across the state in the past eight years.
Texas and New Jersey, meanwhile, have boards that regularly examine such deaths.
“California is flying blind without a state regulatory agency that has meaningful enforcement authority. It’s time to correct this institutional failure,” said Ross Mirkarimi, the former San Francisco sheriff who is now a jail consultant. “It is a perfect opportunity for the governor to arc from the era of realignment into a new period of reform for California jails.”
Sen. Nancy Skinner, D-Berkeley, chairs the California Senate Public Safety Committee. She voted in support of realignment in 2011, when she was in the Assembly. Skinner said “there’s a lot of frustration” about how passive the state board has been in overseeing county jails.
“The sheriffs do have the authority here, and they could do the right thing,” Skinner said in an interview. “We as the state definitely have to improve our oversight.”
Gov. Gavin Newsom’s office, in a written statement, said Kern County’s jail practices are unacceptable, and local officials should reform their policies.
“County jails should not hold people in their custody in isolation indefinitely, no matter what the situation is,” the governor’s statement reads. “This is troubling, and it is this Administration’s hope that the findings in the reports issued by the Board of State and Community Corrections will catalyze change and reforms at the local level, where authority to make those changes ultimately resides.”
Many local jails across the country use variations of suicide watch to remove hazards and increase monitoring of vulnerable inmates. But Kern County uses isolation far more aggressively, and often exclusively, to prevent suicide deaths. “In my career, this is how suicide watch is done,” said Chief Deputy Tyson Davis, the jails’ top administrator. “They go into a cell by themselves with as few points to hurt themselves on as possible.”
That runs counter to best practices advocated by mental health experts, who are increasingly critical of isolating and stripping people considering suicide. A growing body of research shows the practice can harm a person’s mental health and actually increase their suicide risk once they are released from watch.
Youngblood, the sheriff, declined multiple interview requests, and his office declined to discuss specific cases, including Taylor’s.
After McClatchy and ProPublica asked questions about Kern County’s isolation practices and its use of yoga mats, the sheriff’s office replaced the mats with blankets that are resistant to rips. And Davis said in September that he is working to add mental health specialists to inmate screening, which deputies alone have long conducted. The new clinical positions are not funded yet.
Bill Walker, Kern County’s behavioral health director, is in charge of mental health care in the jails. When asked in August if isolation without clinical treatment is harmful, Walker replied, “I would be the first to agree with you.” However, he continued, Kern County’s suicide watch is better than the indifference institutions inflicted decades ago on the people they detained.
“We used to bury people in the state hospitals in unmarked graves,” Walker said. “The humanity of safety is to keep them alive.”
This account is based on interviews with Kern County’s top jail administrators and deputies, county behavioral health directors, former inmates and families of the deceased. The sheriff’s office took reporters on tours of its jail facilities and to see the suicide watch cells. McClatchy and ProPublica also reviewed and analyzed state inspection documents, autopsy reports, court filings, jail purchasing records and state data on in-custody deaths.
An Uptick in Suicides, Then Yoga Mats
In 2011, Lorena Diaz tried to end her life by jumping off a highway bridge. She survived, and a county mental health clinic released her, apparently no more stable than before.
Desperate, her mother called Diaz’s parole agent to ask for help, to find a place where her daughter would be safe. The agent alerted local police, who promptly arrested and booked Diaz into the downtown Bakersfield jail, according to sheriff’s office records. But within two days of her arrival, staff found the 29-year-old mother hanging from a bed sheet tied to a wall vent.
The death was the first in a string of suicides over the next year: A 42-year-old man charged with crashing into a sheriff’s patrol car cut his wrist with a razor and bled out while his cellmates slept. A 20-year-old murder defendant who told deputies he heard voices hanged himself in an isolation cell.
In response to the suicides, Youngblood and his jail staff began sending far more people to suicide watch cells, records show. The practice continues to this day.
“The tripwire to get on suicide watch is fairly light,” said Lt. Ian Silva, who oversees many of the jails’ day-to-day operations. “We don’t want to take any chances.”
The sheriff’s office also added a new feature to its suicide protocol. In March 2012, the agency purchased 25 blue yoga mats, finance records show, and ordered 109 more in July of that year. The mats are a half-inch of foam designed to cushion people doing floor exercises.
They became the only thing Kern County’s suicidal inmates got to sleep on, besides the cement floor or metal bunk. They were also a signal that isolation was no longer a fleeting experience. People began spending longer periods of time on suicide watch.
In state prisons, at-risk inmates receive mattresses. Silva said the sheriff’s office chose to give yoga mats instead to ensure inmates cannot impede deputies from entering cells. “Our big concern with full mattresses is barricading,” Silva said.
Because people with suicidal thoughts often spend their time searching for methods to end their lives, jail experts say suicide watch cells should not contain anything a person can use to asphyxiate or cut themselves.
Kern County deputies violated that rule in August 2013, after deputies booked Luis Campos on a stack of domestic violence charges. Campos had tried to kill himself before, so deputies put him in the watch cell closest to their desk.
The aging facility’s air-conditioning system regularly faltered in the summer, internal investigation records show. So deputies rigged up a portable fan with an extension cord and duct tape to blow air at their watch station as the afternoon heat topped 90 degrees.
They found Campos dead during morning rounds two days later, dangling from the cell bars, an extension cord noosed around his neck.
Until last year, the sheriff’s office had only 11 specialized suicide watch cells across its three jail facilities, and they were always full. So deputies began using what are called safety cells as suicide watch overflow.
Safety cells are closet-sized rooms with nothing but four walls and a grate in the floor. No bed. No water fountain or toilet. They’re temporary storage boxes for people who’ve lost control.
California jail standards say safety cells should only hold inmates who are damaging the building or showing an active intent to hurt themselves or others. Medical staff members are required to evaluate each inmate within 12 hours, and a jail administrator needs to reapprove holding them in the safety cell every 24 hours thereafter.
By early 2015, Kern County’s jail deputies were sending nearly three dozen people a week to suicide watch, a 29% increase from a year earlier. Some were removed from watch in hours. Others stayed for days.
Still, elsewhere in the jails, the suicides continued. That January, a 31-year-old man hanged himself. He’d first tried to kill himself days earlier, a nearby inmate later told detectives. The following September, a 25-year-old man with a history of depression died the same way in a group cell after telling his parents he would kill himself if they did not bail him out.
Deputies said they were unaware that either posed a suicide risk, according to autopsy records.
Meanwhile, state inspectors from the corrections board made their routine tours of Kern County’s jails and reviewed their internal records every two years. By the time an inspector arrived in June 2016, 10 inmates had taken their lives in 5 1/2 years. The inspector did not mention the deaths in the reports. And in evaluating safety cells, one of the reports simply noted “documentation for the use of those cells were good.”
Two more men hanged themselves in January and February 2017, as deputies sent upward of 36 inmates a week to isolation cells.
Christine Taylor was soon among those on suicide watch.
“When Am I Going to Get Out?”
Keys banging on the door woke her that first morning.
“Taylor!” the deputy making the morning rounds shouted. She crawled from underneath the cell bed, where she had been hiding from the lights, and moved toward the metal door. She looked out the smudged plexiglass window. It was like peering through a porthole on a space shuttle, she said.
The person on the other side wouldn’t open the door. Kern County jail staff almost never do during these routine cell checks and brief behavioral health evaluations. So Taylor crouched on her knees and spoke to the specialist through the food-tray slot in the door. She said she was not suicidal. She was only on suicide watch, she pleaded, because she hadn’t cooperated with deputies during intake.
“When am I going to get out?” Taylor asked as the staffer walked away.
“Well,” she heard, “we’ll see.”
Police had arrested her on suspicion of elder abuse. Her father, who suffers from Alzheimer’s disease, claimed that she attacked him during a middle-of-the-night disagreement. But Taylor, then 47, had video showing the opposite; in fact, officers had responded to similar calls at their home before, for offenses imagined or badly misunderstood. This time, deputies refused to watch the tape.
Now Taylor was alone, a dozen yards from the deputy desk. She tried to sleep. It was the only thing to do — inmates on suicide watch in Kern County don’t get books to read or recreation time to interact with other inmates because even that could be too dangerous, sheriff’s officials said.
So she covered her eyes from the light with her clothes and rolled up her yoga mat to use as a pillow. About four hours crawled by after she entered the jail when staff returned to the door and said they were moving her.
For a moment, Taylor felt a rush of excitement. She thought about all the things this might mean: a pillow, a toothbrush, a shower, maybe even a cellmate, someone to talk to.
Deputies instead led her around the corner to another suicide watch cell, next to a deputy’s desk. The furnishings were the same: bed, toilet and yoga mat. But the move shortened the distance the deputies had to walk as they signed off on the required twice-every-30-minutes checks. And she could see staff and inmates walking out of the elevators past the window. There were people around, Taylor thought, people to hear about how she’d been wronged.
“Innocent until proven guilty!” she screamed, calling out to other inmates to join her protest. No one did. “I didn’t get my phone call! I didn’t get my phone call!” Taylor chanted.
Her confusion had given way to resentment. There was nothing the jailers could do to her that would be worse than being in that cell, she thought, so Taylor vowed to make everybody in earshot hear her outrage. She’d become part of the collective wail that greeted her just hours earlier.
Jail staff ignored her.
Taylor tried another tactic: She ripped a piece of material from her paper-thin shirt and fashioned it into a small nooselike loop. She said she dangled it in the porthole window. (Jail staff wrote that she put it around her neck, sheriff’s office records show.) Deputies stormed the cell and restrained her, Taylor said, and records show staff replaced the clothes with a hunter green, tear-resistant suicide smock.
The following day, around noon on Tuesday, jail records show deputies transferred her to a punishment cell, known as administrative segregation.
“If They’re Committed, It’s Hard to Stop Them”
Kern County’s behavioral health department doesn’t provide treatment to inmates on suicide watch, aside from dispensing medication for previously diagnosed conditions, said Walker, the department’s director. Last year, the county agency doubled its jail staff, which now employs about 40 caregivers.
Counties usually have a written agreement with the behavioral health provider working in the jails. The contract — among the most foundational parts of jail-medical operations — dictates what the provider will do, as well as the consequences for failing to deliver services. But in Kern County, the jail has had no such agreement for “several years,” Walker said. That means there’s no written accountability for when things go wrong. County officials maintain a contract isn’t necessary.
The behavioral health department does not reliably track how many people have attempted suicide in the cells, why people were placed in isolation or how long they stayed, he said. It also does not keep data on inmates sent to outside hospitals because of mental illness.
After every death of a mentally ill inmate, behavioral health and jail staff meet to review the case and determine if there are ways to prevent similar fatalities in the future. However, officials have not examined the jails’ suicide deaths as a whole at any point since 2011, Silva and Walker confirmed.
During an interview in August, the county’s top behavioral health officials demurred when asked why Kern County’s jail suicide deaths had increased dramatically.
“I don’t think I have an answer I could give you at the moment,” Walker said. Deputies don’t send all suicidal inmates to behavioral health staff. Greg Gonzales, head of correctional care, said suicide prevention cannot keep all inmates safe. “If they’re committed, it’s hard to stop them,” he said.
At the sheriff’s office, Silva partly attributed the increased deaths to “bad luck.”
The behavioral health department provides inmates the best care it can afford, Gonzales said.
Over the past two decades, researchers have examined suicides in local jails, where death rates are often higher than among the general public and in prisons. They’ve consistently opposed the use of isolation, saying it increases the likelihood that inmates will attempt to hurt themselves. A guide from the World Health Organization states, “Prisoners at risk should not be left alone, but observation and companionship should be provided.”
The key to keeping people safe in local jails is paying attention, said Sheriff Tom Dart from Cook County, Illinois, whose Chicago-area jails are increasingly a model for humane practices. Dart said he eliminated isolation as punishment when his department’s data showed the practice actually led to more rule violations and security problems.
“If you value something as a society, you study it,” Dart said. “You analyze it. You spend money on the data. If you don’t care about something, you don’t study it.”
A 2014 statistical analysis of New York City’s jail inmates found serious mental illness and solitary confinement were the strongest factors in suicide attempts.
Lindsay Hayes, a national expert on correctional suicide prevention, said jails use isolation with good intentions. “I truly believe that correctional officials and mental health and medical officials and leadership are not intentionally trying to punish people, to create tortuous types of environments,” Hayes said. “They’re just being extremely careful and, in many ways, over-protective and over-reactive.”
A “Lonely Cell” and Endless Daylight
Taylor felt worlds away from another human being. In the punishment cell, around the corner from suicide watch, no one walked by. She couldn’t hear voices or the clatter of activity. Distance muted everything.
“It was the loneliest feeling I’ve ever had,” she said. “That feeling is what made me decide that I wanted to be good and go back to the cell behind the deputies.”
The “lonely cell,” as she called it, broke her in less than a day. She apologized. She told deputies she’d learned her lesson. More importantly, Taylor said, “I was just being quiet.”
Deputies moved her back to the suicide watch cell by the desk that Wednesday morning, two days after being booked into the facility, according to jail records.
She tried to measure the hour by watching how much sunlight streamed onto the jail hallway floor. Peering through the window, she learned to tell time by making mental notes about when one deputy’s shift ended and another person’s began.
She marked the hours with scraps of food and shreds of a paper plate, but it was all guesswork. The constant light triggered sleep deprivation and confusion. Taylor had lost track of just how long she’d been in Kern County’s jail.
Bedbugs, Yoga Mats and a Shrug
In California, this kind of isolation is entirely permissible.
To bolster oversight of county jails and distribute funds in the realignment era, state lawmakers created the corrections board. Every two years, it sends an inspector to each facility to make sure sheriffs and their officers are following the rules.
Steven Wicklander, an inspector for the state board, arrived at the Kern County jails in June 2018, a year after Taylor’s arrest. The central receiving jail was in the midst of a bedbug infestation. The sheriff’s staff was not regularly cleaning cell mattresses, Wicklander wrote in his notes. They handed out dirty beds and only washed them when the mattresses were “contaminated.”
Conditions weren’t much better in the newest jail, opened last year and built with $100 million in state funds to cope with an influx of inmates serving longer sentences in county facilities under realignment. Its expansive infirmary is primarily for suicide prevention, and its 14 isolation cells were constantly full.
Over three days, Wicklander toured the suicide watch halls at each jail facility. He saw maxed-out cells and deputies putting suicide watch inmates in safety cells for more than a week straight.
“The safety cell cannot be used as a substitution for treatment,” Wicklander wrote in his final report in August 2018.
There were violations at every stop. Kern County jails are so understaffed the sheriff’s office requires deputies to work overtime to cover the shifts, causing deputies to fall behind on safety and security checks. Suicide watch and safety cell practices, particularly the yoga mats, were against the rules.
Agency officials do not have authority to make county leaders change and generally see themselves as partners, not regulators, said Allison Ganter, deputy director overseeing the inspection team.
“We are not enforcement,” she said.
Youngblood and his staff waited eight months to respond to Wicklander’s report.
They wrote back this April and rejected the board’s findings that yoga mats violated the standards. The sheriff’s office spent $4,500 to buy 60 more mats the same month, finance records show.
Yoga mats, they wrote, provide people on suicide watch “the comfort of padding, albeit minimal, in an environment which is uncomfortable by design.”
A New Caregiver, and a Long Walk Home
As the week went on, Taylor tried to talk to anyone who walked by her cell. Once, a woman sat near her window, and they chatted briefly about being arrested and their legal cases. “She was telling me her story, which was almost like my story,” Taylor recalled.
She tried to get the staff talking. Taylor said she noticed a picture of a puppy on a deputy’s monitor and complimented the pet’s cuteness. The deputy scolded her and turned the screen away.
“The most exciting part of the day was when they would give me my food because there was actually somebody there,” Taylor said.
Saturday marked her sixth day in the jail. That morning, a different behavioral health specialist met with Taylor and decided that her suicide risk — however deputies calculated it initially — was gone. She moved to a space with the rest of the inmates in the jail’s general population ward, where she was thrilled to receive a toothbrush, soap, clothes and a mattress.
Deputies also gave her access to a phone for the first time since she’d been put on suicide watch early Monday morning. Taylor called her mom, who helped arrange for her to post the $35,000 bond. (Two weeks later, prosecutors dropped the charges. Taylor sued the county for wrongful detention, but the suit was dismissed.)
The sheriff’s office said it is not permitted to discuss her case under state law and would not answer reporters’ questions about her time in jail.
It can take hours to be formally released from custody, and oftentimes inmates are released in the middle of the night without reliable transportation. Late Sunday, the doors of the downtown Bakersfield jail swung open for Taylor. A 4-mile walk in the dark awaited her.
She had been in sweats when police arrested her and didn’t have a bra to wear for the trek home. Taylor asked if she could borrow one of the jail-issued ones.
“It’s bad luck to take anything home from here,” a deputy replied.
“Good advice,” she said.
If you or someone you know needs help, here are a few resources:
Call the National Suicide Prevention Lifeline: 1-800-273-8255
Text the Crisis Text Line from anywhere in the U.S. to reach a crisis counselor: 741741