We’ve been advised to wash our hands more frequently in the current coronavirus outbreak, but should we be looking at keeping our smartphones cleaner too?
Coronavirus is spreading, and fast. Since it first infected humans in late 2019 there have been thousands of cases and hundreds of deaths. In our globalised world, it is easy for a very contagious virus, like Covid-19, to spread so it’s useful to know what practical steps we can take to keep ourselves safe. Our phones are our digital companions, they come with us everywhere and can host germs of all kinds. Here are three simple steps to help you reduce the potential coronavirus risks from your smartphone:
1. Clean your phone regularly
Several studies have shown that our phones are dirtier than our toilet seats and potentially host more germs. When was the last time you cleaned your phone? Not a quick wipe to clean the screen, but actually cleaning it with a dedicated surface cleaner? Our phones are hotbeds of germs. In taking a phone call you’re putting that bacteria on your face, and by not washing your hands before you snack you’re putting those bacteria in your mouth. We suggest cleaning your phone regularly, at least once a day, in order to stay free of those germs which you pick up in everyday life and which then stay on your phone, even after you wash your hands.
Experts have suggested that alcohol wipes, rather than soap and water, are the most effective way to keep your smartphones clean.
2. Don’t put your phone down
This might sound like contradictory advice coming from Time To Log Off! But we’re not suggesting you stay on your phone – we’re suggesting you don’t put your phone down on a surface in a public place. Don’t place it on a table in a coffee shop or bar for example, because you don’t know who’s been there before. The World Health Organisation does not yet know how long Covid-19 can survive on surfaces but they assume a few hours to a few days.
3. Be careful what you believe online
Once again, fake news has raised its ugly head around an international incident. Since the outbreak of coronavirus, there has been a deluge of inaccurate information online including lists of various quack ‘cures’. Our advice is to only trust reputable, verified, news sources such as the BBC, or WHO for your news and information about how to avoid catching coronavirus, as well as what might happen to you if you did.
There’s a more significant connection between smartphones and coronavirus than you might think. Our phones are our constant companions so they can potentially even impact our health in terms of catching viruses not just impact on our sleep. Keep yourself safe by following our tips, and hopefully, it will help us all to develop more hygienic habits along the way too.
While hand-washing is preferred, hand sanitizers with at least a 60% alcohol concentration can be an effective alternative to always using soap and water, but only if your hands are not visibly soiled.
Editor’s note: The World Health Organization has declared that COVID-19, the disease caused by the new coronavirus, has a higher fatality rate than the flu. As of March 4, 2020, nine deaths have been reported in the U.S. Brian Labus, a professor of public health, provides essential safety information for you, from disinfectants to storing food and supplies.
1. What can I do to prevent becoming infected?
When people are sick with a respiratory disease like COVID-19, they cough or sneeze particles into the air. If someone is coughing near you, the virus could easily land on your eyes, nose or mouth. These particles travel only about six feet and fall out of the air rather quickly. However, they do land on surfaces that you touch all the time, such as railings, doorknobs, elevator buttons or subway poles. The average person also touches their face 23 times per hour, and about half of these touches are to the mouth, eyes, and nose, which are the mucosal surfaces that the COVID-19 virus infects.
We public health professionals can’t stress this enough: Proper hand-washing is the best thing you can do to protect yourself from a number of diseases including COVID-19. While hand-washing is preferred, hand sanitizers with at least a 60% alcohol concentration can be an effective alternative to always using soap and water, but only if your hands are not visibly soiled.
The best way to wash your hands.
2. Wouldn’t it be easier just to clean surfaces?
Not really. Public health experts don’t fully understand the role these surfaces play in the transmission of disease, and you could still be infected by a virus that landed directly on you. We also don’t know how long the coronavirus that causes COVID-19 can survive on hard surfaces, although other coronaviruses can survive for up to nine days on hard surfaces like stair railings.
Frequent cleaning could remove the virus if a surface has been contaminated by a sick person, such as when someone in your household is sick. In these situations, it is important to use a disinfectant that is thought to be effective against the COVID-19 virus. Although specific products have not yet been tested against COVID-19 coronavirus, there are many products that are effective against the general family of coronaviruses. Cleaning recommendations using “natural” products like vinegar are popular on social media, but there is no evidence that they are effective against coronavirus.
You also have to use these products properly in accordance with the directions, and that typically means keeping the surface wet with the product for a period of time, often several minutes. Simply wiping the surface down with a product is usually not enough to kill the virus.
In short, it isn’t possible to properly clean every surface you touch throughout your day, so hand-washing is still your best defense against COVID-19.
3. What about wearing masks?
While people have turned to masks as protection against COVID-19, masks often provide nothing more than a false sense of security to the wearer. The masks that were widely available at pharmacies, big-box stores and home improvement stores – until a worried public bought them all – work well at filtering out large particles like dust. The problem is that the particles that carry the COVID-19 virus are small and easily move right through dust masks and surgical masks. These masks may provide some protection to other people if you wear one while you are sick – like coughing into a tissue – but they will do little to protect you from other sick people.
N95 masks, which filter out 95% of the small, virus-containing particles, are worn in health care settings to protect doctors and nurses from exposure to respiratory diseases. These masks provide protection only if they are worn properly. They require special testing to ensure that they provide a seal around your face and that air doesn’t leak in the sides, defeating the purpose of the mask. People wearing the mask also must take special steps when removing the mask to ensure that they are not contaminating themselves with the viral particles that the mask filtered out. If you don’t wear the mask properly, don’t remove it properly or put it in your pocket and reuse it later, even the best mask won’t do you any good.
4. Should I stockpile food and supplies?
As a general preparedness step, you should have a three-day supply of food and water in case of emergencies. This helps protect from disruptions to the water supply or during power outages.
While this is great general preparation advice, it doesn’t help you during a disease outbreak. There is no reason to expect COVID-19 to cause the same damage to our infrastructure that we Americans would see after an earthquake, hurricane or tornado, so you shouldn’t plan for it in the same way. While you don’t want to run out of toilet paper, there is no reason to buy 50 packages.
A Wuhan-type quarantine is extremely unlikely, as a quarantine won’t stop the spread of a disease that has been found all over the world. The types of disruptions that you should plan for are small disruptions in your day-to-day life. You should have a plan in case you or a family member gets sick and you can’t leave the house for a few days. This includes stocking up on basic things you need to take care of yourself, like food and medicines.
If you do get sick, the last thing you are going to want to do is run to the grocery store, where you would expose other people to your illness. You shouldn’t wait until you are out of an important medication before requesting a refill just in case your pharmacy closes for a couple days because all their employees are sick. You also should plan for how to handle issues like temporary school or day care closures. You don’t need to prepare anything extreme; a little common-sense preparation will go a long way to make your life easier if you or your loved ones become sick.
Voters have frequently complained that the debate has been confusing and hard to follow. Here are six things to know as you tune in to the increasingly frenzied primary race.
Health has been a top issue in the presidential campaign during the past year: Not only do the Democratic candidates disagree with President Donald Trump, but they also disagree among themselves.
Voters have frequently complained that the debate has been confusing and hard to follow. Most of the attention so far has been focused on whether the U.S. should transition to a “Medicare for All” program that would guarantee coverage to all U.S. residents — and result in higher taxes for most people. But there is far more to the health debate than that.
The campaign is nearing some key moments — the caucuses in Iowa next week, the New Hampshire primary Feb. 11, voting in Nevada and South Carolina later in the month. By March 3, Super Tuesday, Democrats will have chosen a third of all delegates.
Here are six things to know as you tune in to the increasingly frenzied primary race.
Universal coverage, Medicare for All and single-payer are not all the same thing.
Universal coverage is any method of ensuring that all of a country’s residents have health insurance. Other countries do it in various ways: through public programs, private programs or a combination.
Single-payer is a system in which one entity, usually but not always a government, pays for needed health care services. Single-payer is NOT the same as socialized medicine. The latter generally refers to a system in which the government pays all the bills, owns the health facilities and employs the health professionals who work there. In a single-payer system, such as Medicare in the U.S., the bills are paid by the government but the delivery system remains mostly private.
Medicare for All is a proposal that was originally developed in the late 1980s. Building on the popularity of the Medicare program for senior citizens, the idea was originally to extend that program to the entire population. However, since Medicare’s benefits have fallen behind those of many private insurance plans, the later iterations of Medicare for All would create an entirely new, and very generous, program for all Americans.
Voters are more concerned about health care costs than health care coverage.
While Democrats fight over how best to cover more people with insurance, the majority of Americans already have coverage and are much more worried about the cost. A recent survey of voters in three states with early contests — Iowa, South Carolina and New Hampshire — found voters in all three ranked concerns about high out-of-pocket costs far ahead of concerns about insurance coverage itself.
It’s the prices, stupid.
There’s a good reason voters are so concerned about what they are being asked to pay for medical services. U.S. health spending is dramatically higher than that of other industrialized nations. In 2016 the U.S. spent 25% more per person than the next highest-spending country, Switzerland. Overall U.S. health spending is more than twice the average of other Western nations.
But that’s not because Americans use more health services than citizens of other developed nations do. We just pay more for the services we use. In other words, as the late health economist Uwe Reinhardt once famously quipped in the title of an academic article, “It’s the Prices, Stupid.” A later paper published last year (the original is from 2003) confirmed that is still the case.
Drug companies and insurers aren’t the only ones responsible for high prices.
To listen to many of the candidates’ messages, it may seem drug companies and health insurers are together responsible for most — if not all — of the high health spending in the U.S.
“The giant pharmaceutical and health insurance lobbies have spent billions of dollars over the past decades to ensure that their profits come before the health of the American people,” says Sen. Bernie Sanders on his presidential campaign website. “We must defeat them, together.”
Most insurance spending, though, actually goes for care delivered by doctors and hospitals. And some of their practices are far more gouging to patients than high prices charged by drugmakers or administrative costs added by insurance companies. Wall Street firms that have bought physician groups are helping block a legislative solution to “surprise bills” — the often huge charges faced by patients who inadvertently get care outside their insurance network. And hospitals around the country are being called out by the news media for suing their patients over bills almost no patient can afford.
Democrats and Republicans have very different views on how to fix health care.
To the extent health has been covered in the presidential race, the story has been about disagreements between Democrats: Some want Medicare for All, while others are pushing for less sweeping change, often described as a “public option” that would allow but not require people to purchase a government health plan.
There are much bigger divides between Democrats and Republicans, however. Democrats nearly all support a larger role for government in health care; they just disagree on how much larger it should be. Meanwhile, Republicans generally want to see less government and more market forces brought to bear. The Trump administration has already either implemented or proposed a variety of ways to decrease regulation of private insurance and is weighing whether to allow states to effectively cap their Medicaid program spending.
And in the biggest difference of all for the coming campaign, the Trump administration and a group of GOP-led states are, again, challenging the entire Affordable Care Act in court, arguing that it is unconstitutional based on the 2017 tax law’s zeroing out of the tax penalty for failing to maintain insurance coverage.
The Supreme Court has opted not to decide the case in time for the 2020 election, but it is likely to continue to be a major issue in the campaign.
There are important health issues beyond insurance coverage and costs.
While Medicare for All and drug prices have dominated the political debate during the past year, other critical health issues have received far less attention.
Some candidates have talked about long-term care, which will become a growing need as baby boomers swell the ranks of the “oldest old.” Several have addressed mental health and addiction issues, a continuing public health crisis. And a few have laid out plans for the special needs of Americans in rural areas and those with disabilities.
HealthBent, a regular feature of Kaiser Health News, offers insight and analysis of policies and politics from KHN’s chief Washington correspondent, Julie Rovner, who has covered health care for more than 30 years.
Season 3 of our digital detox podcast, It’s Complicated, launches today.
Featuring interviews with Love Island’s Dr Alex, Made in Chelsea’s Jamie Laing and Rita’s Quilt’s Sharon Downey
It’s Complicated: Untangling the Relationship With Our Phones, returns today with Season Three of our digital detox podcast. Kicking off with guest Dr Alex of Love Island and Good Morning Britain, the podcast sees award-winning digital entrepreneur, author and Founder of Time To Log Off, Tanya Goodin, navigate the confusing and sometimes controversial subject of our relationships and habits with technology.
Our first episode, featuring Dr Alex George, lands today. Currently working as a frontline doctor in the A&E department at the University Hospital Lewisham in London, Dr Alex chats about the impacts of online media on mental health, with a wide-ranging discussion on his life online before and after the villa, and the tragic loss of Caroline Flack.
Since we launched it last year, the podcast has hosted the likes of Instapoet Nikita Gill and Hinge founder Justin McLeod, sharing and discussing their insights into and personal experience of, achieving a healthy day-to-day balance with tech.
What’s Next for our Digital Detox Podcast?
This series the digital detox podcast will continue to do just that with an exciting variety of guests, including Jamie Laing of Made in Chelsea, Cindy Gallop, founder of the sex tech website MakeLoveNotPorn and Badass Cross Sitch’s creator Sharon Downey. Throughout all ten episodes our guests each bring their unique perspective of the impact the digital world is having on their lives: talking about what tech can give us, and what it can take away.
While each guest has been chosen for their unique angle on our relationship with tech, we hope that each and every episode will reassure listeners how common unhealthy relationships with phones really are. The realisation that bad tech habits negatively impact our lives might even help listeners to come together to figure out how to develop healthy relationships with smartphones. We launched our digital detox podcast to stimulate the conversations that might help us all do just that. Season Three is available from 2 March 2020.
What are the different pressures faced by Anita Hill and Christine Blasey Ford regarding their testimonies of alleged sexual and gender mistreatment by Supreme Court Justices Clarence Thomas and Brett Kavanaugh?
As the founder of the #MeToo movement, why is Tarana Burke, a black woman, getting death threats from black men?
The underlying core of these questions is: What really makes trauma traumatic?
Decades of research on trauma, or physical, sexual or psychological violence, have shown the same thing: Victimization hurts people. Sexual assault in particular can be painful to all who experience it.
However, as a trauma expert who has studied the effect of violence for over a decade, I have found that there is a unique harm for black people and other minorities whose perpetrators are of the same minority group.
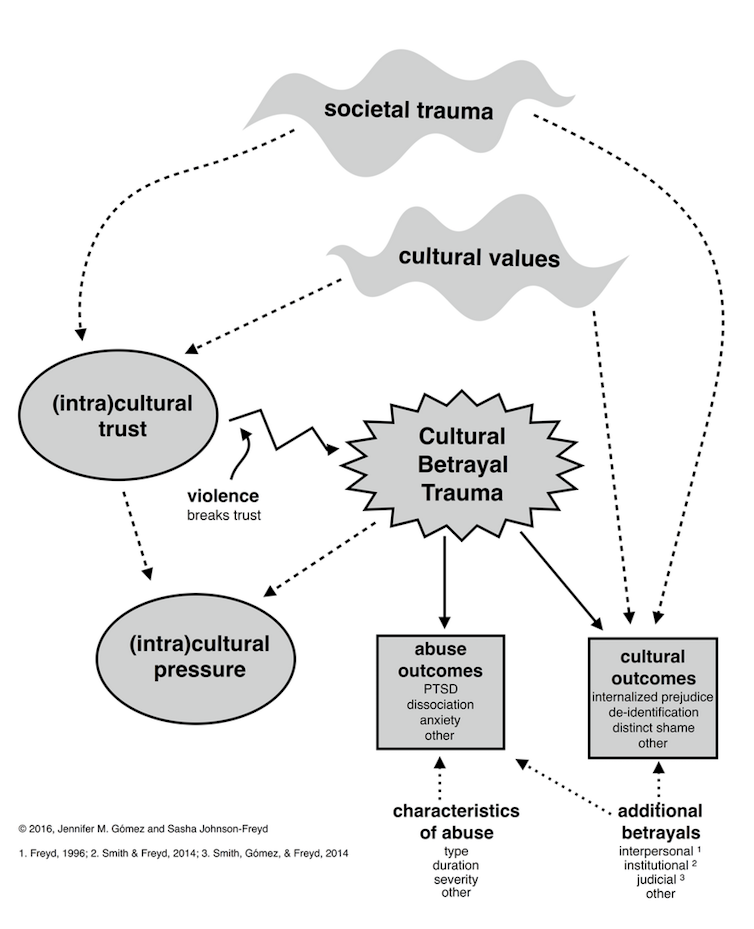
To understand this harm, I created cultural betrayal trauma theory. The general idea of cultural betrayal trauma theory is that some minorities develop what I call “(intra)cultural trust” – love, loyalty, attachment, connection, responsibility and solidarity with each other to protect themselves from a hostile society. Within-group violence, such as a black perpetrator harming a black victim, is a violation of this (intra)cultural trust. This violation is called a cultural betrayal.
The Harms of Cultural Betrayal
Cultural betrayal leads to many different outcomes.CC BY-SA
Cultural betrayal trauma, which is simply within-group violence in minority populations, is associated with many outcomes that go beyond things that are typically studied with trauma, such as post-traumatic stress disorder. It includes some things not often thought about with trauma, such as internalized prejudice – like a black person believing the stereotype that all black people are violent.
(Intra)cultural pressure is another outcome of cultural betrayal trauma. With (intra)cultural pressure, people who experience cultural betrayal trauma are often demanded to protect the perpetrators and the minority group as a whole at all costs, even above their own well-being. With the mandate of “don’t betray your race,” (intra)cultural pressure punishes people who speak out about the cultural betrayal trauma they have endured.
In a recent study, I tested cultural betrayal trauma theory in youth due to the increased risk for trauma and mental health problems in the transition into adulthood.
I surveyed 179 college women online in 2015. Over 50% of these young women were victims of trauma. Just under half experienced psychological violence, 14% endured physical violence, and almost one in three women were victims of sexual violence.
Of the young women who were victimized, over 80% reported at least one form of (intra)cultural pressure. This included their ethnic group suggesting that what happened to them may affect their minority group’s reputation. An example of this could be a black woman who has been raped by a black man being told that she should not go to the police because it will make all black people look bad.
Additionally, I found that controlling for age, ethnicity and interracial trauma, cultural betrayal trauma and (intra)cultural pressure were associated with symptoms of PTSD. Meaning, cultural betrayal in trauma and (intra)cultural pressure were unique contributing factors of mental health problems in ethnic minority college women.
What Does This All Mean?
As I analyzed the findings, I was struck by several things:
The within-group nature of trauma includes a cultural betrayal in minorities that affects mental health.
Trauma gives us only part of the picture.
Group-level responses and cultural norms via intra-cultural pressure impact mental health.
Policy change that combats inequality, such as changes in education, health care, law enforcement and the judicial system, can benefit minorities who experience trauma.
These findings have implications for interventions. Such therapy can address the very real threats of discrimination and the necessity for (intra)cultural pressure. At the same time, these interventions can use (intra)cultural trust to promote positive mental health. Additionally, evidence-informed feminist approaches, such as relational cultural therapy, may benefit people who are exposed to both trauma and societal inequality.
The body of research to date suggests that cultural betrayal may be a unique harm within violence in minority populations, including the black community. As such, the alleged sexual traumas perpetrated by R. Kelly and Clarence Thomas have a cultural betrayal that isn’t found in Woody Allen’s alleged abuse. Moreover, black men’s death threats against Tarana Burke are (intra)cultural pressure that is laced with misogynoir, or sexism in the black community.
Research that incorporates societal inequality can help us understand what makes trauma traumatic. In doing so, our social reactions and therapeutic interventions can ultimately be effective for blacks and other minorities who are exposed to trauma.
Users have been concerned about the impact of screentime on our mental and physical health since the creation of the WorldWideWeb. We’ve trawled through the records to show you that the history of anxiety about screens, and attempts to spend time off them, is as long as the history of screens itself.
The History of Digital Detox:
1998
With the creation of the WorldWideWeb in the early-90s researchers (primarily psychologists and anthropologists) first started to suggest that it might not be a wholly beneficial invention, with the early emphasis being on the “overuse” phenomena and internet addiction and dependency. Dr Kimberley Young penned: ‘Caught in the net: how to recognize the signs of Internet addiction–and a winning strategy for recovery‘, and proposed one of the first sets of criteria to detect Internet addiction. Any individual who fulfilled five of the following eight criteria would be regarded as Internet addicted:
Preoccupation with the Internet;
A need for increased time spent online to achieve the same amount of satisfaction;
Repeated efforts to curtail Internet use;
Irritability, depression, or mood lability when Internet use is limited;
Staying online longer than anticipated;
Putting a job or relationship in jeopardy to use the Internet;
Lying to others about how much time is spent online; and
Using the Internet as a means of regulating mood.
2008
China became the first country in the world to classify ‘internet addiction disorder’ as a mental illness. Since then the government estimates 24 adults and children have been diagnosed and over 300 military-style bootcamps have sprung up all over the country to enforce drastic and draconian digital detox methods.
2009
When early social media platforms launched in the early-00s; LinkedIn (2002), YouTube (2005), and MySpace (2003), concerns shifted to the impact these types of applications might be having on our brains. A group of researchers produced a paper entitled: ‘Social network and addiction’, indicative of the worry social media addiction was beginning to cause.
2012
A study found that around 60% of Facebook users had made a conscious effort to voluntarily take a break from Facebook for a time period of several weeks or more. This early form of digital detox was referred to the as ‘media refusal’, with non-users known as ‘social media rejectors’.
Camp Grounded launched its first digital detox retreat in California with 10 guests.
2013
Former Googler Tristan Harris launched the Center for Humane Technology, formerly called Time Well Spent, to spread awareness and talk about the aspects of technology that are often ignored, such as attention and distraction and their effects on the user
2014
Our founder, Tanya Goodin, responded to the growing concerns coming from North America and Asia about our excessive attention to screens and founded Time to Log Off in the UK. We’ve spent the past six years collecting research and resources on the subject to share with our community.
2015
A survey conducted by Deloitte found that around 59% of smartphone users checked a social media platform in the five minutes before going to bed, and within 30 minutes of waking up.
A 2015 review concluded there was a probable link between basic psychological needs and social media addiction. “Social network site users seek feedback, and they get it from hundreds of people—instantly. It could be argued that the platforms are designed to get users ‘hooked‘.”
The first digital detox retreat was run by Time To Log Off in Europe, in October of this year.
2016
A reduced sense of wellbeing was found in teenagers who passively, rather than actively, used social media. Research by Chassiakos, Radesky, and Christakis showed that the manner of social media use was the key factor, rather than the amount of time engaged. A decline in well-being and life-satisfaction was found in older adolescents who passively consumed social media, but these were not found in those who were more actively engaged.
2017
Facebook admitted that this passive consumption of social media, described in the 2016 research, could be harmful to mental health, although they said active engagement could have a positive effect. An Oxford University study showed that digital use can be seen as conforming to a ‘Goldilocks effect‘ – with both spending too much and too little time on screens having a negative impact on wellbeing. It suggested that moderate use could have positive effects in terms of connectivity, which we have always pointed out at Time to Log Off.
Our first book, Off: Your Digital detox for a Better Life was published, one of the very first titles looking at the reasons for digital detox – and how to do one, and is now translated into seven languages.
2018
An Organisation for Economic Co-operation and Development (OECD) report noted the benefits of ‘structured and limited’ internet use in children and adolescents for developmental and educational purposes, but found that excessive use could have a negative impact on mental wellbeing, leading to discussions about what excessive use looked like and what form breaks from screens should take.
2019
Radesky and Christakis, published research which suggested that there are developmental risks when young children have too much access to screens too early. There was also a review of the research carried out to date and though there have been various methodical critiques the conclusion was that there are concrete connections between screen time and health problems, whilst limited use led to some social benefits. Researchers also found that a majority of adults in the US use Facebook and 60% of those have made an active effort to use it less in recent times.
Clearly we’re just at the beginning of our relationship with the digital detox. As concerns about excessive time spent on screens grows, so to is the impulse to want to spend more time away from them. We’re committed to spreading information and resources to anyone who wants to get better tech:life balance. Join us and sign up to our community to get all the latest information and research as it becomes available.
A North Carolina rehab program promised recovery, free of charge, to people struggling with drug addiction. When they arrived, they were put to work without pay at adult care homes for the elderly and disabled.
Jennifer Warren has spent years recruiting the poor and desperate to her drug rehabilitation program in the mountains outside Asheville, North Carolina.
She promised them counseling and recovery for free. When they arrived, she put them to work 16 hours a day for no pay at adult care homes for the elderly and disabled.
Thrust into the homes with little training or sleep, the rehab participants changed diapers, bathed patients and sometimes dispensed the same prescription drugs that sent them spiraling into addiction in the first place.
For some, the temptation proved too great. They snorted prescription pain pills, swallowed droplets of morphine from used medical syringes and peeled fentanyl pain patches off patients and sucked them to get high.
Then there were the allegations of assault. At least seven participants from Warren’s program, Recovery Connections Community, have been accused of sexual misconduct or assault of patients at the homes. Former participants and workers said no one reported the incidents to social services, as required by law. The accused continued working or were simply transferred to another care home.
“There’s a whole lot in the program that’s covered up,” said Charles Polk, who completed Warren’s program in 2017 for alcohol addiction. “The only thing she thinks about is the money.”
Charles Polk of Monroe, N.C., completed the Recovery Connections program last year. He says the program’s director, Jennifer Warren, thinks only about money. Credit: James Nix for Reveal
Amid a nationwide opioid epidemic, treatment remains out of grasp for most people struggling with addiction. Those with wealth and insurance often are able to pay thousands of dollars for private long-term programs. But the less fortunate have become easy prey for rehabs with a tantalizing promise: freedom from addiction for free.
To pay for their stay, participants must work full-time jobs and surrender their pay. An ongoing investigation by Reveal from The Center for Investigative Reporting has found that many programs exploit this arrangement, providing few actual services while turning participants into indentured servants.
In North Carolina, Warren has turned her nonprofit rehabilitation program into her personal empire. She worked the people in her program to exhaustion, while regularly vacationing in places such as Paris, Greece and New Orleans for Mardi Gras, according to former participants and state records. She diverted nonprofit donations meant for the program – appointments at beauty salons and concert tickets – to herself and used participants’ food stamps to stock her own kitchen.
In addition to working at adult care homes, the 40 or so men and women in Warren’s program have baby-sat her children, cared for hundreds of her exotic pets and cleaned her house.
“It’s like slavery,” said Denise Cool, who was addicted to crack cocaine when a judge ordered her to the rehab in 2011, “like we were on the plantation.”
Jennifer Warren is shown in a 2015 booking photo after she was caught illegally collecting thousands of dollars’ worth of food stamps. Credit: Buncombe County Bureau of Identification
Even after being stripped of her counseling license in 2012, Warren continued to operate her program with impunity. Authorities from four separate state agencies neglected complaints, botched investigations and stood by for years as Warren flouted rules they were supposed to enforce.
It was not until Reveal questioned state officials about their inaction that they began taking steps to curb the abuses.
Warren, who is 52 years old, declined to answer questions from Reveal.
“I have no reason to believe that you will report anything positive about our program or are interested in the people’s success stories, of which there are many,” Warren wrote in an email.
When confronted by a former participant in a private Facebook message in February, Warren responded, “It’s so easy to buy into the negativity.”
“Because of the structure of this kind of program, many people leave with resentments and are disgruntled,” she wrote in the message, obtained by Reveal. “I have spent the majority of my adult life trying to give back.”
Founded in 2011, Recovery Connections Community has grown to include three locations, run from rural homes near Asheville and Raleigh.
Hundreds of people have sought help from Recovery Connections over the years. Many are sent there by the courts as an alternative to prison. Others come directly from hospitals, mental health facilities and state-funded detox centers.
Whitney Richardson was addicted to heroin and facing prison time for burglary when a North Carolina judge ordered her to complete the two-year program in 2014 as part of a plea agreement.
Judges and probation officers weren’t supposed to use unlicensed rehabs such as Recovery Connections for treatment. And the rehab specifically had been on probation officials’ radar. In internal emails, one official said it was “a bad agency and is run by dangerous people.”
Richardson fled four months later. She was so scarred by the experience that she vowed never to attend rehab again. When she later relapsed, she said she got herself clean by buying Suboxone on the street.
“It’s not right to take advantage and subject people to abuse like that when they’re trying to better their lives,” Richardson said. “No one should ever go to that place.”
***
Jennifer Warren – known then as Jennifer Hollowell – was working on a doctorate at the University of Alabama when she got hooked on crack cocaine.
She dropped out of her clinical psychology program and at 27 years old checked herself into a residential rehab program in Winston-Salem that required that she and other participants work for free.
Warren flourished in the rehab, becoming the director’s assistant once she graduated. “I wanted to be like her, and she became my role model,” she would later recall.
But in 2002, after the director left amid allegations that she had stolen money and – former employees said – dated a client, Warren and several other clients decided to start a program of their own. They called it Recovery Ventures.
With her flowing blond hair and colorful dresses, Warren projected the image of a free spirit. She described clients as family and would invite them to socialize in her home, which was adorned with fairy figurines and painted bright purple inside.
“She could just look at you and just read straight through you, I swear to God,” said former client Lakindra Edwards. “Like, wow. She don’t even know me, but she told me everything about me.”
But Warren soon began to cross ethical lines. She instructed her clients to clean her home and care for her growing collection of llamas, miniature ponies and exotic birds. Then she, too, began a romantic relationship in 2008 with a client she was counseling.
Phillip Warren would spend the night at her house, and they would kiss around other clients. Dating a participant violated a host of state ethics rules, but when friends and colleagues tried to intervene, Jennifer Warren crumpled into tears.
Undeterred, she moved up Phillip Warren’s graduation date and moved him into her house. The two married years later.
By 2011, multiple complaints about Jennifer Warren had reached the North Carolina professional licensing board. In the official document later filed against her, the board chastised her for her ethical breaches and said she wasn’t cut out for the rehab business. In fact, the more time patients spent around her, the licensing board wrote, the more likely they were to relapse.
Warren “used and exploited her clients for her personal benefit” and “failed to maintain appropriate boundaries between herself and her clients,” the board wrote. The state eventually revoked her counseling license.
The rehab fired her in 2011. A few days later, Warren struck out on her own, founding Recovery Connections. To pay for her program, she turned to a handful of employers always in need of workers: adult care homes.
***
Rachel Thomas was working one night in 2016 at Candler Living Center, a home near Asheville for mentally ill and disabled adults, when a worker from Jennifer Warren’s program came sprinting down the hall.
An elderly resident was gasping for air and repeatedly vomiting. Thomas discovered that the rehab worker – who was not trained to dispense prescription drugs – had given the patient the wrong medication.
“He actually about killed one of the residents,” said Thomas, who no longer works at Candler. “He had no idea what was going on.”
A former employee at Candler Living Center, a facility for mentally ill and disabled adults outside Asheville, N.C., contracted with Recovery Connections for workers. It houses nearly 30 residents. CREDIT: NANCY PIERCE FOR REVEAL
Participants from Recovery Connections worked in at least nine homes over the years. Some worked as janitors and cooks, but the majority worked as personal care aides.
In North Carolina, personal care aides must receive at least 80 hours of training, during which they learn how to safely feed, lift and bathe patients. But many rehab workers interviewed by Reveal said they never received the training required by law. Some Recovery Connections participants also dispensed medication with no training, even though state law requires a special certification.
“I would die if someone like that was taking care of my mom,” said Renee Thayer, a former program participant who was assigned to work as a personal care aide in 2012.
The rehab workers cost the facilities less than regular employees. Some homes paid Recovery Connections the minimum wage – $7.25 an hour – for each worker and did not pay workers’ compensation, insurance or overtime, according to former managers and internal records obtained by Reveal.
Disasters Happened All the Time
One employee at Hominy Valley Retirement Center would unlock the medicine cart and place pain pills into white paper cups. Then, rather than take the prescription drugs to the residents herself, she would order the rehab workers to pass out the pills while she slept on a recliner, said Charles Polk, a former participant who also dispensed the drugs.
“Lots of people relapsed and got high that way,” he said. “They stole the meds. They would just take it.”
Fentanyl pain patches, which slowly release an opioid up to 50 times more powerful than heroin, were in particularly high demand. When it was time to shower patients in chronic pain, some rehab workers would peel off the patches and keep them for themselves.
“They would take their patches off them and suck the fentanyl out,” said Ian Hays, a former manager at Recovery Connections. “One girl told me, ‘I got high every day in the fucking program.’ ”
***HELP US REPORT THIS STORY We’re trying to figure out how many work-based rehabs there are in the United States. Fill out this form if you know about one. And email us if you’re a journalist or news organization that wants to report on rehabs near you.***
At least seven rehab workers have been accused of sexual assault or misconduct with patients at the homes. Former employees said none of the allegations were reported to authorities, as required by law. Reveal could find no mention of any of the alleged assaults in thousands of pages of police reports, Adult Protective Services records and county and state inspections. The accused continued working or simply were transferred to other facilities.
One male rehab worker was accused of sexually assaulting a disabled elderly woman in the shower at Candler in 2016. After the incident, the woman refused to let the rehab worker shower her.
“I don’t want him to do it!” she cried while pointing at the worker, recalled Polk, who witnessed the interaction.
In response, Candler barred male rehab workers from bathing female residents, according to seven current and former employees and participants. As of mid-May (2018), the man still was working at the home.
Chris Damiani, chief executive officer of the company that owns Candler and Hominy Valley, said his agency had never had problems with rehab workers. He said that none of the alleged assaults were reported to management and that his company was investigating the issues raised by Reveal’s reporting.
“We do not take any report of abuse, neglect, assault, theft or drug use lightly,” Damiani said.
Cedarbrook Residential Center, an assisted-living facility in Nebo, N.C., houses 80 residents and used workers from Recovery Connections Community. Credit: Nancy Pierce for Reveal
In 2014, another rehab worker was accused of sexually assaulting a disabled woman in her bedroom at Cedarbrook Residential Center, the woman and four former employees said.
She said she fought him off and immediately reported the incident, but the administrator “plumb out ignored me.”
“I hated the place,” said the woman, who left the facility in 2016. “I felt like I was literally in hell.”
Frederic Leonard, Cedarbrook’s owner, said the facility never filed a formal report with the county Department of Social Services because the facility conducted its own investigation and concluded that an assault had not occurred. He declined to provide more details about the internal investigation.
“We have safeguards in place to prevent misconduct of this type,” he said. “It is difficult when mentally ill adults, who are suffering from severe mental illness, are also poor historians of fact.”
The accused worker continued to work at the facility for several days. His presence terrified the patient who had accused him, she and a former employee said.
At Recovery Connections, Warren dealt with the alleged assault in her weekly therapy group. Rather than call police, she placed the man in the middle of a circle while his peers screamed at him and called him a sexual predator, according to two former participants.
“They all went off on him,” said Blake Loving, who attended the therapy session. “He just sat there.”
After the session, Warren sent the accused worker to another care home.
“It was really sick,” said Whitney Richardson, who also attended. “They just kind of wanted to brush it under the rug.”
***
Jennifer Warren collects a salary of about $65,000 a year, according to tax filings, but that money alone never seemed to be enough. For years, she has used her rehab’s nonprofit status as a vehicle for personal enrichment.
Every day, a group of Warren’s clients said they were expected to make hundreds of phone calls to businesses and major corporations asking them to donate goods and services, according to state records, former participants and staff. They asked Tommy Hilfiger for designer clothes, Hilton for hotel stays and The Cheesecake Factory for free meals. Warren used the nonprofit to score free concert tickets to see her favorite bands.
Jennifer Warren’s Trips
The donations were tax deductible and were supposed to go to program participants. But Warren got first pick of everything.
“Jennifer and them got all the good stuff,” said Jessica Stanley, who attended the rehab in 2016 and called businesses on the program’s behalf. “It was a little hustle-scam.”
Participants routinely called nail and hair salons to book free appointments. They said the salon visits would help rehab participants “build their self-esteem.” But Warren was the one who showed up.
“She was taking advantage of all the donated manicures and pedicures,” said Ian Hays, the former Recovery Connections manager. “She used to go to one place in the mall all the time.”
During one appointment, a hairstylist asked Warren how long she had been in the program, according to a former staff member who witnessed the interaction and records from a state investigation. When Warren admitted she was the founder, the stylist was livid.
Warren also ordered program participants to sign up for food stamps, which former participants said she used to stock her own kitchen.
In 2015, Warren pleaded guilty to financial assistance fraud for lying about her income and illegally collecting thousands of dollars’ worth of food stamps. She was sentenced to 45 days of probation. But participants say she continued to use their benefits to fill her personal pantry.
While Warren got steaks, participants said they often were left with little more than Hamburger Helper, crackers and tubs of peanut butter. At times, they complained there was no food at all.
“Sometimes we ate ramen noodles at night,” recalled Roshawnda McIllwain, a former participant who left the program last year. “Some days, I went hungry.”
But there was always money for animals.
Warren spent more than $32,000 in program funds on animal expenses, according to the nonprofit’s tax filings from 2014 and 2015.
She bought goats and sheep at animal auctions around the country. She had two arctic foxes, large ostrich-like birds called rheas and sugar gliders – small marsupials that resemble flying squirrels. Warren claimed they were for the rehab’s animal therapy program.
“Some people collect stamps. Some people collect shoes. Jennifer’s got a thing for collecting animals,” said Hays, the former manager.
Warren keeps dozens of them at her home in Black Mountain, participants said. Her bedroom is stacked with cages of toucans and other tropical birds.
At one of Recovery Connections’ outposts near Raleigh, an entire barn is crammed with animals, according to participants. Guinea pigs tumble over each other in crates. Rats multiply by the dozens. Inside a dimly lit garage, monkeys languish in cramped cages. Several participants recalled burying dead llamas in the program’s yard.
Even though the program had horses for its “equine therapy program,” participants said they weren’t allowed to ride them.
Julia Harris said she was struck with one thought when she checked herself into the program in 2017.
“I have landed in an insane asylum,” she remembers thinking. “I’m in a filthy house with animals and animal fur. And this is supposed to be a rehab?”
Julia Harris, pictured at her home near Brevard, N.C., said she was struck with one thought when she arrived at Recovery Connections last year for help with an alcohol problem: “I have landed in an insane asylum.” Credit: James Nix for Reveal
***
For some people, the worst part of Jennifer Warren’s program was not the work at the care homes or the personal chores – it was the therapy groups.
The sessions usually occurred at Warren’s house. The group sat in a large circle of folding chairs and loveseats while each person took a turn in “the hot seat” in the middle. The other patients then cursed, screamed and hurled insults at the person for up to 45 minutes at a time.
Spoiled brat.
Stupid bitch.
Motherfucking whore.
Participation was mandatory. People frequently broke down crying. Some participants said Warren and others seemed to relish it.
“You see certain people planning this shit all week, looking for stuff to use against you,” said Scott Hucks, who left the program in 2016. “It’s like a joke, it’s like a game. Just entertainment.”
Sometimes, Warren would black out the windows and keep a select group awake for days on end as they recited their life stories. If anyone started to doze off, participants said they were sprayed with water. Some people said they began to hallucinate.
“It’s like CIA torture,” said Heather Fox, who left the program last year.
Warren said the groups were meant to teach participants conflict resolution skills. They learned how to confront the harshest realities of their lives and move past it, she explained in a deposition for a 2010 lawsuit brought by a client who found her first rehab, Recovery Ventures, abusive.
“I wouldn’t say it’s verbal abuse,” she said. “It’s an incredible healing opportunity.”
“Is there screaming involved?” the lawyer asked her.
“Sometimes,” Warren replied.
Warren’s therapeutic tactics are rooted in a drug rehab program called Synanon, which was founded in 1958. Studies have shown that the group sessions, which involve screaming and insults, can be catastrophic for people with poor mental health and low self-esteem. Law enforcement officials later denounced the program as a cult.
Most participants interviewed by Reveal said they found Warren’s therapy sessions humiliating. Those who complained were punished with more work. They were forced to scrub floors with a toothbrush or cut grass with a pair of scissors.
“They wanted us to be so broken down emotionally that we would listen to whatever they said,” said Heather Teatzner-Brown, who attended the rehab for alcohol addiction and fled in the middle of the night in 2016. “Just take it and not have an opinion or your own mind.”
Some former participants interviewed by Reveal spoke positively about the program, saying Warren and her rehab were there for them when no one else was.
“If you’re at a crossroads in your life and you’ve burned up every bridge out there, it’s the best way,” said Rick Taylor, who graduated in 2014 and credits it with helping him overcome a drug addiction. “All I had to do was just surrender and do what I was told.”
Others left the program worse off than when they arrived. Some turned to drugs to cope. Many participants told Reveal that they fled into the mountains, sometimes in the rain or snow or in the middle of the night.
“I was physically sober, but my mind was way worse than it ever was before when I was using,” recalled Tommy Farwick, who attended the program in 2012. “I had zero desire to live anymore. I just wanted to die.”
Through all this, Warren demanded that people work around the clock because the more they worked, the more money they brought in for the rehab.
“Y’all need to make some money,” Hays recalled her saying.
***
North Carolina regulators were well aware of the abuse at Recovery Connections.
Soon after Jennifer Warren opened in 2011, the Department of Health and Human Services received a complaint alleging that she was operating an unlicensed rehab program, in violation of state law. In North Carolina, any facility offering 24-hour treatment is required to be licensed.
When investigator Joy Allison arrived at Recovery Connections to check it out, Warren greeted her warmly. Even though Warren was advertising her program as “substance abuse treatment” online and in brochures, she told Allison a different story: She was running halfway houses, not a treatment program.
Allison accepted that explanation and then offered Warren a tip: If she said she was operating a “12-step, self-help” program, Warren could avoid state oversight completely. Warren used the new language on promotional materials but changed little else.
Seven years later, that decision continues to allow Warren to operate her rehab free of government oversight. But the complaints haven’t stopped: forced labor, self-dealing and abuse.
Each time, Allison gave the same answer. “I have continued to receive calls/complaints about this program but, have explained that they are exempt from licensure,” she wrote in an internal email in 2016.
After questions from Reveal, the state health department finally began to crack down.
On May 16th 2018 it banned Recovery Connections from sending participants to work as caregivers at adult care homes, potentially cutting off the program’s main source of funding. The department said Recovery Connections must be licensed as a staffing agency to continue dispatching workers.
But the department said the program still is not required to be licensed as a drug rehab center.
Recovery Connections has escaped accountability from other state agencies as well.
Since 2011, the North Carolina secretary of state’s office has received complaints that Warren has pocketed donations meant for the program. Its investigators conducted a full investigation, speaking with business owners who had been defrauded by Warren and reviewing internal call logs and financial documents.
But the agency ultimately dropped the case. Its reason: Participants never sent officials signed and notarized affidavits.
Recovery Connections got to keep its charitable solicitation license and nonprofit status, which allows Warren to continue to collect tax-deductible donations from businesses and the public.
In exasperated emails to authorities, the directors of several licensed rehab centers expressed their dismay that Warren kept dodging accountability.
“This individual believes that the rules do not apply to her, no matter how many warnings or disciplinary actions are taken,” David Martin, who had co-founded Warren’s first rehab with her, wrote to the attorney general’s office in a July 2012 email.
Martin ticked off her latest transgression. Warren “spent the entire month of June at the beach” and used the rehab’s food stamps for herself, he wrote. Was this something the attorney general would pursue?
An investigator promised to look into it, but nothing came of it.
The North Carolina Department of Public Safety had its turn to crack down around the same time. Probation officers began hearing complaints in 2012 from people who had been ordered by the court to go to Recovery Connections.
In internal emails, probation officials agreed that the program was unsuitable for offenders and griped about Warren’s sordid history. But they continued to allow probationers to attend.
“We are not responsible for policing the agencies available to the offenders,” one administrator wrote in an internal email.
Following questions from Reveal, probation officials finally took action against the rehab.
“We have determined that the Recovery Connections locations do not align with our mission, vision, or goals,” the department wrote in a May 8 memo (2018). Going forward, no probationer will be allowed there.
But hospitals and short-term treatment centers continue to send people to the program. So do social workers at state-funded detox and psychiatric facilities. Recovery Connections is always willing to accept those who have nowhere else to go.
Jennifer Warren is waiting for them.
More from the All Work. No Pay. series Read: Impact: Officials take action on rehab work camp in response to Reveal investigation Read: They thought they were going to rehab. They ended up in chicken plants Read: Inside a judge’s rehab: Unpaid work at a local Coca-Cola plant Read: Response to work camp investigation: ‘Nothing short of slavery’
We talk all the time about being ‘on’ 24:7. We have to check our emails: we never know what might come up during the lunch break which requires immediate attention. We have to have our notifications on: what if we missed the release of tickets for our favourite artist? We have to be on Twitter all the time or we might miss the next trending topic and be behind the breaking news story. Living like this is draining. UK adults now spend an average of 8 hours and 41 minutes a day on screens – more time than we’re asleep! People often ask us what an achievable way to do a digital detox might look like. So here’s one idea for trying a digital detox: living 24:6.
What is 24:6?
The idea of living 24:6 is to be be just as accessible as usual, apart from one day a week. Typically this day would be Sunday, after all, it is the day of rest. However, you could pick Wednesday to split up the week, or Monday so that it starts a bit better, whatever works for you. You can choose exactly what form 24:6 takes for you personally too. Perhaps you need a break from email but watching a little TV with the kids could be a nice relaxing way to wind down in the evening and bond? You might choose to give up social media but still check your phone messages. Or you could go cold turkey, no phone, no screens of any kind, and have one day where you can just breathe. We can guarantee that you will appreciate the break!
If the point of living 24:6 is to put less stress on yourself then you might want to take a few steps beforehand so it doesn’t stress you out even more! If you won’t be contactable then talk to those for whom it’s important to be able get hold of you. You could give them a landline number or the number of someone you’ll be with. It can be hard to commit to a new habit so make it as easy for yourself as possible by thinking through and eliminating problems up front.
Give 24:6 living a go, maybe for just this week, and let us know how you get on? We love to get your feedback about what is working for you in trying a digital detox and building a more mindful lifestyle. Good luck!
Valentine’s Day. Whether we view it as a holiday on a par with Christmas, or snub it as another money-making invention by card companies, it’s hard to ignore the opportunity to do something to show our loved ones how much we care.
However, no matter how wonderfully thoughtful the plans you have made for Valentine’s Day, they won’t be complete if you’re glued to your screen. To really participate in Valentine’s Day we need to be present and fully in the moment with our loved ones.
Unsurprisingly, research has found that the more often someone gets ‘phubbed‘ (phone snubbed) by their partner, the less satisfied they are with their romantic relationship. With Valentine’s Day approaching, we need to figure out how to get our technology use under control so that it doesn’t have a negative impact on our relationships.
Valentine’s Day is about making your significant other feel special. How can you do this when you refuse to give them your full attention? We need to learn to live through each other, and not through our screens. This is why every year we run our #logoffforlove campaign.
6 Do’s and Don’ts to #logoffforlove this Valentine’s Day
DO Write a card
Whilst sending a quick text to let your partner know how much you appreciate them requires less planning, it just can’t beat the feeling of receiving a card. Knowing that you have invested time and attention into picking out a card and then filling it with a meaningful message will make your partner feel miles more special than any emoji ever could.
DO Put your phone away during dinner
Spending time together requires more than just being sat on the same table at a restaurant. Dinners together can be a wonderful way to take a break from our hectic lives and spend quality time together, but checking your phone throughout dinner signals that you are not fully invested in your partner. Give them your full attention; put it on do not disturb so that even the buzzing of notifications won’t be a distraction.
DO Choose a screen-free activity
Whilst movies are great, wouldn’t it be nice to interact with the other a little more? Even if you are concentrated on the same thing, having your eyes fixed to a screen, with parallel lines of sight, does not invite the same intimacy and affection that other activities would. Do something like cooking together, or go for a walk: anything that involves face-to-face communication and interaction.
DON’T check social media
Again, you’re spending time together, so why would you want to shift your focus onto what others are doing at this moment? In fact, many even find that their partner’s love of social media feels like there is a third person in the relationship. Show your partner that you are fully invested in them by not allowing them to become a third wheel to you and your phone.
DON’T check your phone before bed
Having your phone in the bedroom is just not a good idea. It compromises your sleep, is not exactly an aphrodisiac, and checking it before bed yet again signals to your partner that you are more interested in other people’s lives and stories right now than theirs.
DO Continue this all year
These tips aren’t just for Valentine’s Day – they’re great habits to adopt in order to establish a healthier relationship with our tech. We need to be reminded to prioritise our human relationships. These steps should be good starting points towards overcoming our addition to our phones. Good luck, and have a Happy Valentine’s Day.
Digital detox is what we do. We write about the benefits of time away from screens and put it into practice with our retreats and our founder’s public and private talks. But digital detoxes aren’t the only way to experience the benefits of screen-life balance, there are new trends every day including of late the idea of a dopamine fast. What’s that? Well, we’ve done the work for you to explain what a dopamine fast is, how to do one, and what you can get out of it.
What is dopamine fasting?
Dopamine is a neurotransmitter which creates motivation in the brain for various activities such as exercise, talking and TV. It rewards us for behaviours which we find enjoyable and so tells us that they are worth repeating. In the time before tech that was fine, it’s good to want to swim, talk, read or run more; but the tech CEOs of Silicon Valley have taken it one step farther by deliberately creating software which gives us a dopamine hit. So, dopamine fasting is a new trend which took off at the end of the last decade to avoid all of those behaviours in order to ‘reset’ your brain. Now, I don’t know about you but the idea of not talking, reading and just sitting inside bored for a weekend doesn’t appeal. Dopamine is a natural chemical so why don’t we just manage our dopamine the way our grandparents did?
How Silicon Valley is changing our brains
We’ve talked before about the ways that tech CEOs make their products ‘sticky‘. This is how they get us to stay on their apps for so long, we’re waiting for a dopamine hit; from a ‘like’, ‘comment’, ‘share’ or even a ‘streak’ on Snapchat. Each time we get one they reinforce our brains to stay on screens and then come back again time and again, in the same way slot machines work at a casino. This wouldn’t be a problem if we didn’t already know about the negative impact of screens on our mental and physical health, with sleep, concentration and creativity being the worst hit. So, if we want to take back control of our brains and redirect our attention to a more fruitful place then we need to rebalance our reactions to screens – maybe by going on a occasional dopamine fast.
How to do dopamine fasting right
The kind of hits we get from social media and technology are fast and repetitive, so we’d recommend for the ideal dopamine fast you do a digital detox and try to replace the time you would be on your phone with slow-release enjoyable activities. But, just taking away your phone may not necessarily limit your dopamine if you spend your time watching TV or playing video games – so try and go properly analogue. Think bored teenager in the 80s! You could go for a swim, read a book or cook a long dinner. Anything away from quick gratification will give you the satisfaction of dopamine but in a far healthier and more productive way than simply a ‘like’. You could even use this time to reset your morning routine or incorporate more elements of reflection and exercise to an already busy life, perhaps a dopamine fast will even help you find time for a new resolution.





 Our first book,
Our first book, 
















{kind=link}